

Chronic Tobacco-Smoking on Psychopathological Symptoms, Impulsivity and Cognitive Deficits in HIV-Infected Individuals
- PMID: 28303534
- PMCID: PMC5529218
- DOI: 10.1007/s11481-017-9728-7
Chronic Tobacco-Smoking on Psychopathological Symptoms, Impulsivity and Cognitive Deficits in HIV-Infected Individuals
Abstract
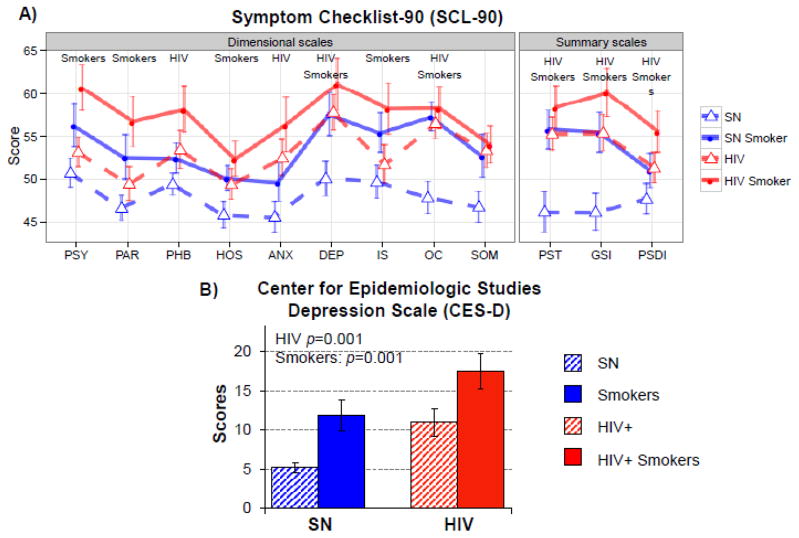
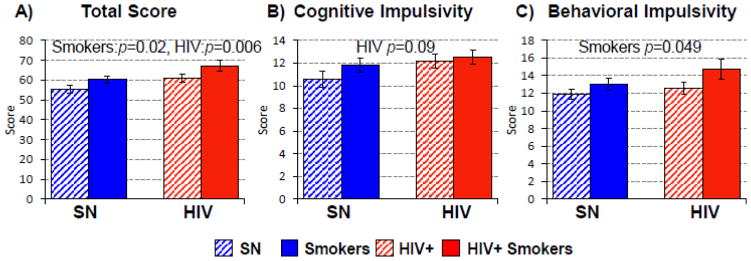
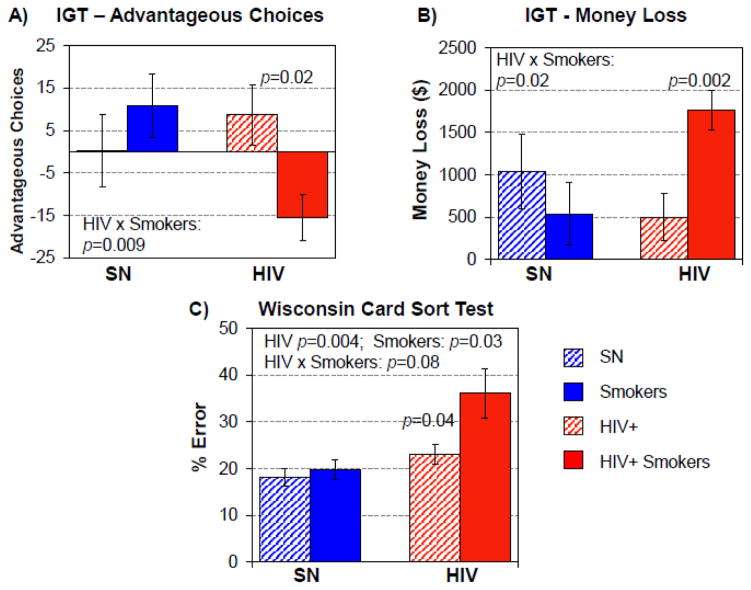
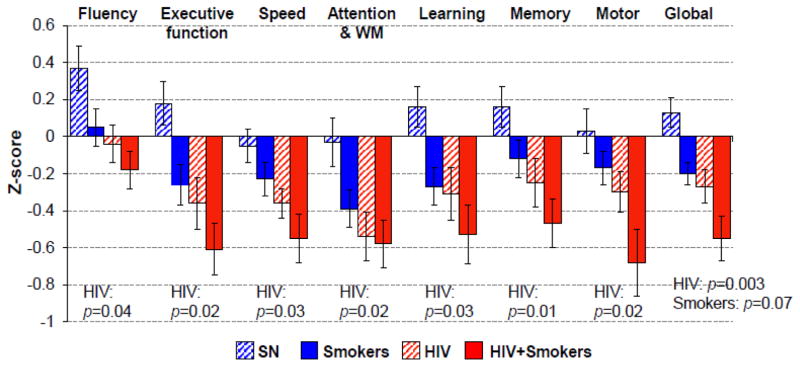
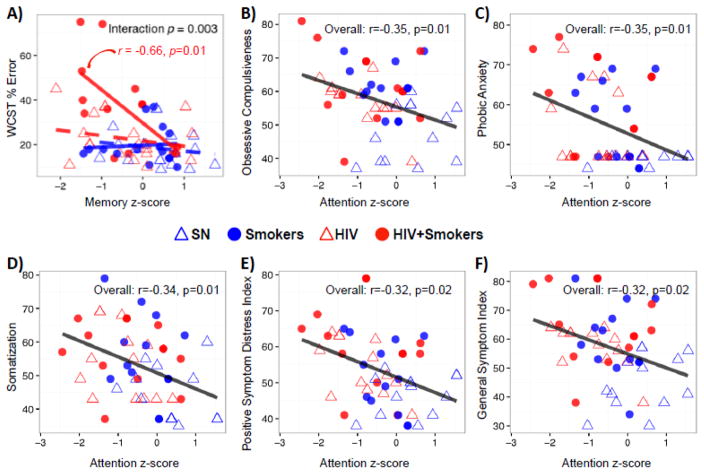
HIV-infected individuals (HIV+) has 2-3 times the rate of tobacco smoking than the general population, and whether smoking may lead to greater psychiatric symptoms or cognitive deficits remains unclear. We evaluated the independent and combined effects of being HIV+ and chronic tobacco-smoking on impulsivity, psychopathological symptoms and cognition. 104 participants [27 seronegative (SN)-non-Smokers, 26 SN-Smokers, 29 HIV+ non-Smokers, 22 HIV+ Smokers] were assessed for psychopathology symptoms (Symptom Checklist-90, SCL-90), depressive symptoms (Center for Epidemiologic Studies-Depression Scale, CES-D), impulsivity (Barratt Impulsiveness Scale, BIS), decision-making (The Iowa Gambling Task, IGT, and Wisconsin Card Sorting Test, WCST), and cognition (seven neurocognitive domains). Both HIV+ and Smoker groups had higher SCL-90 and CES-D scores, with highest scores in HIV+ Smokers. On BIS, both HIV+ and Smokers had higher Total Impulsiveness scores, with higher behavioral impulsivity in Smokers, highest in HIV+ Smokers. Furthermore, across the four groups, HIV+ Smokers lost most money and made fewest advantageous choices on the IGT, and had highest percent errors on WCST. Lastly, HIV+ had lower z-scores on all cognitive domains, with the lowest scores in HIV+ Smokers. These findings suggest that HIV-infection and chronic tobacco smoking may lead to additive deleterious effects on impulsivity, psychopathological (especially depressive) symptoms and cognitive dysfunction. Although greater impulsivity may be premorbid in HIV+ and Smokers, the lack of benefits of nicotine in chronic Smokers on attention and psychopathology, especially those with HIV-infection, may be due to the negative effects of chronic smoking on dopaminergic and cardio-neurovascular systems. Tobacco smoking may contribute to psychopathology and neurocognitive disorders in HIV+ individuals.
Keywords: Decision making; HIV; Psychopathology; Risk; Tobacco use.
Conflict of interest statement
Figures
References
-
- Bechara A, Martin E. Impaired decision making related to working memory deficits in individuals with substance addictions. Neuropsychology. 2004;18:152–162. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
