

Can podocytes be regenerated in adults?
- PMID: 28306565
- PMCID: PMC5511735
- DOI: 10.1097/MNH.0000000000000311
Can podocytes be regenerated in adults?
Abstract
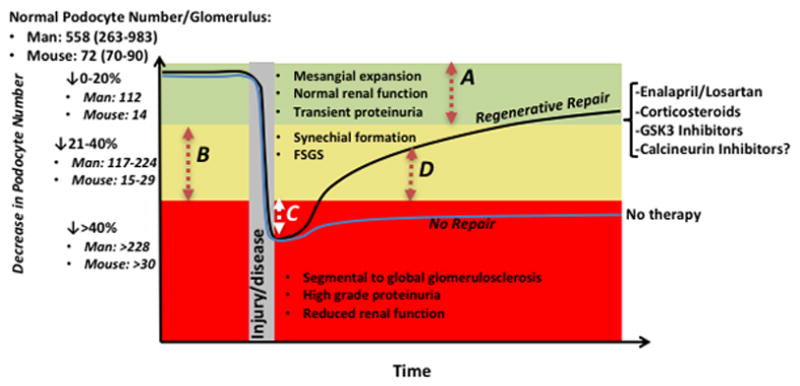
Purpose of review: Podocytes are critical components of the nephron filtration barrier and are depleted in many kidney injuries and disease states. Terminally differentiated adult podocytes are highly specialized, postmitotic cells, raising the question of whether the body has any ability to regenerate lost podocytes. This timely question has recently been illuminated by a series of innovative studies. Here, we review recent progress on this topic of significant interest and debate.
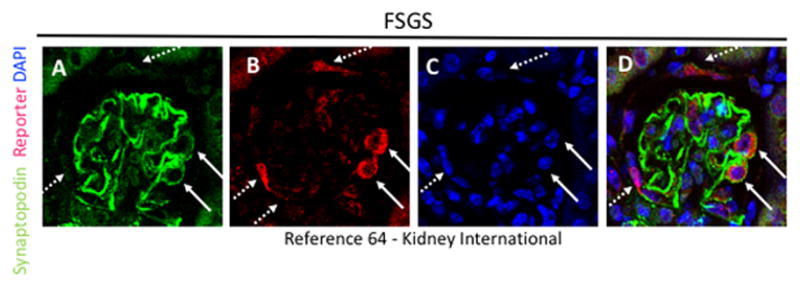
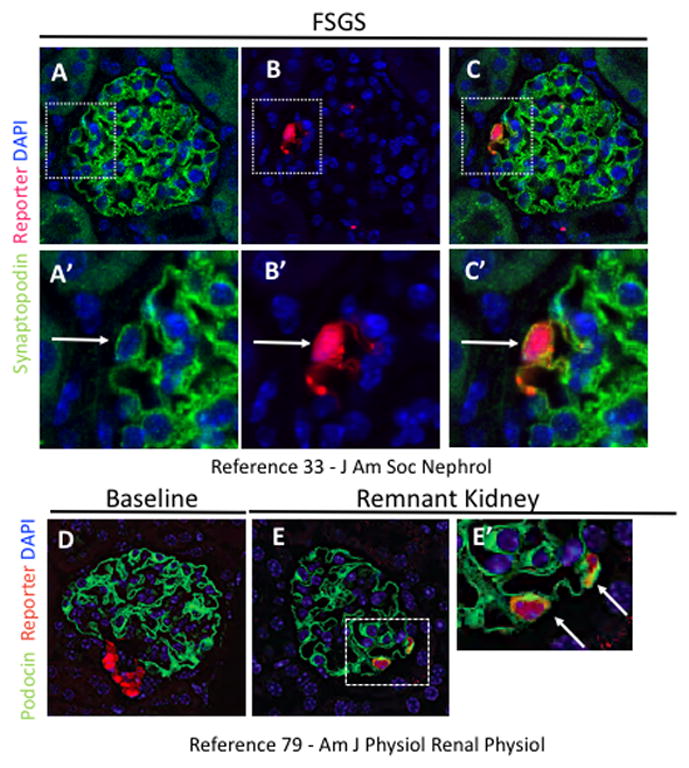
Recent findings: The innovation of genetic labeling techniques enables fate tracing of individual podocytes, providing the strongest evidence yet that podocytes can be replaced by nearby progenitor cells. In particular, two progenitor pools have recently been identified in multiple studies: parietal epithelial cells and cells of renin lineage. These studies furthermore suggest that podocyte regeneration can be enhanced using ex-vivo or pharmacological interventions.
Summary: Recent studies indicate that the podocyte compartment is more dynamic than previously believed. Bidirectional exchange with neighboring cellular compartments provides a mechanism for podocyte replacement. Based on these findings, we propose a set of criteria for evaluating podocyte regeneration and suggest that restoration of podocyte number to a subsclerotic threshold be targeted as a potentially achievable clinical goal.
Conflict of interest statement
Figures
References
-
- Little MH. The Life Cycle of the Nephron Progenitor. Dev Cell. 2015;35(1):5–6. - PubMed
-
- Ashraf S, Gee HY, Woerner S, Xie LX, Vega-Warner V, Lovric S, Fang H, Song X, Cattran DC, Avila-Casado C, Paterson AD, Nitschke P, Bole-Feysot C, et al. ADCK4 mutations promote steroid-resistant nephrotic syndrome through CoQ10 biosynthesis disruption. J Clin Invest. 2013;123(12):5179–5189. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
