

Secondary Endolymphatic Hydrops
- PMID: 28306649
- PMCID: PMC5425947
- DOI: 10.1097/MAO.0000000000001377
Secondary Endolymphatic Hydrops
Abstract
Hypothesis: A review of the most recent literature will provide clinicians with an update of secondary endolymphatic hydrops, aiding in diagnosis and treatment of affected patients.
Background: Secondary endolymphatic hydrops is a pathologic finding of the inner ear resulting in episodic vertigo and intermittent hearing loss. It is a finding for which extensive research is being performed.
Methods: A review of the most recent literature on secondary endolymphatic hydrops was performed using PubMed literature search.
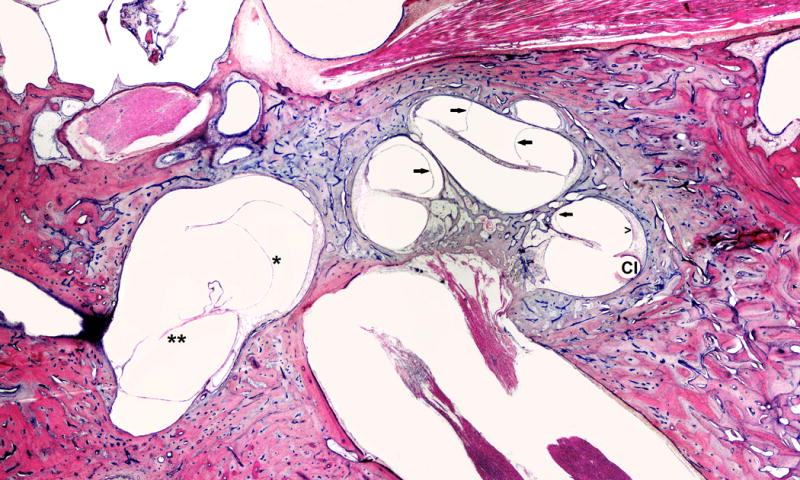
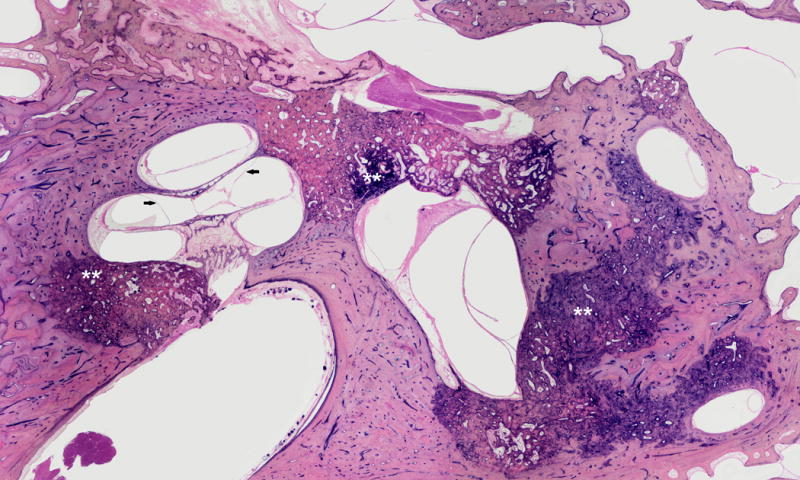
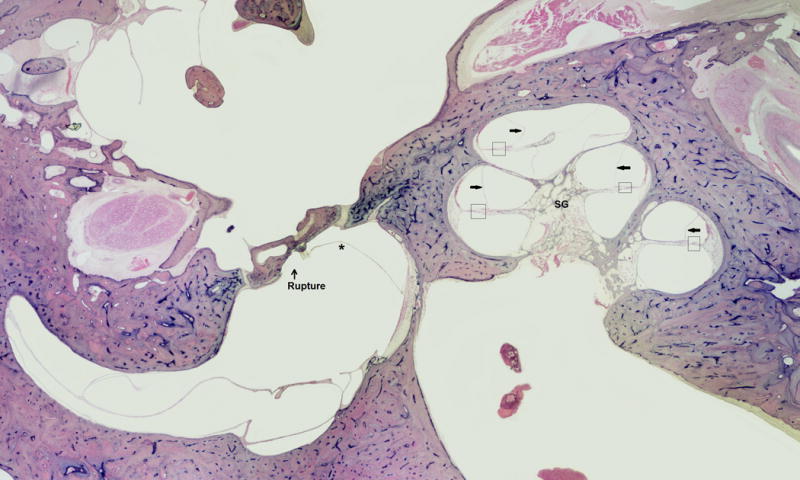
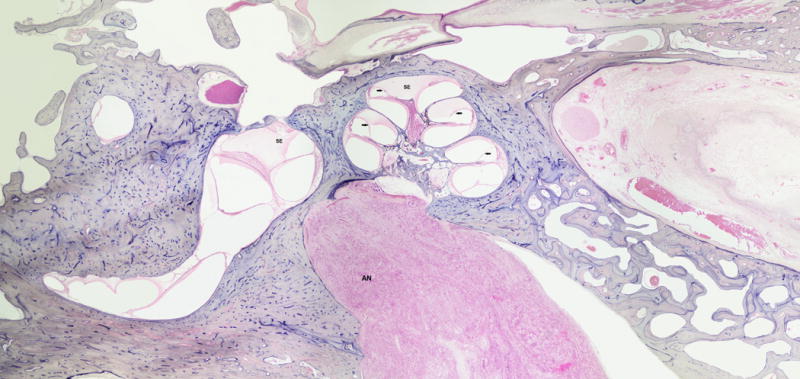
Results: Recent investigation of secondary endolymphatic hydrops has brought attention to traumatic and inflammatory insults as causes for secondary endolymphatic hydrops. Such etiologies, including postsurgical effects of cochlear implantation and endolymphatic sac ablation; otosclerosis and its operative intervention(s); acoustic and mechanical trauma; medications; and systemic inflammatory processes, have been determined as causes of secondary lymphatic hydrops. Histopathological slides for many of the etiologies of secondary endolymphatic hydrops are presented.
Conclusion: Through an understanding of the pathophysiology and etiologies of secondary endolymphatic hydrops, clinicians will gain a better understanding of this complex disease process, which will aid in treatment of patients with this disease process.
Conflict of interest statement
Figures



References
-
- Chen YJ, Young YH. Secondary endolymphatic hydrops after acoustic trauma. Otol Neurol. 2016;36:1–6. - PubMed
-
- Fontaine N, Chapiot A, Debry C, Gentine A. A case of spontaneous intracranial hypotension: from Meniere-like syndrome to cerebral involvement. Euro Ann Otorhinolaryngol Head Neck Dis. 2012;129:153–6. - PubMed
-
- Smeds H, Eastwood HT, Hapson AJ, Sale P, Campbell LJ, Arhatari BD, Mansour S, O’Leary SJ. Endolymphatic hydrops is prevalent in the first weeks following cochlear implantation. Hearing Res. 2015;327:48–57. - PubMed
-
- Handzel O, Burgess BJ, Nadol JB. Histopathology of the peripheral vestibular system after cochlear implantation in the human. Otol Neurotol. 2006;27:57 e64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
