

Cigarette smoking and cardio-renal events in patients with atherosclerotic renal artery stenosis
- PMID: 28306749
- PMCID: PMC5357000
- DOI: 10.1371/journal.pone.0173562
Cigarette smoking and cardio-renal events in patients with atherosclerotic renal artery stenosis
Abstract
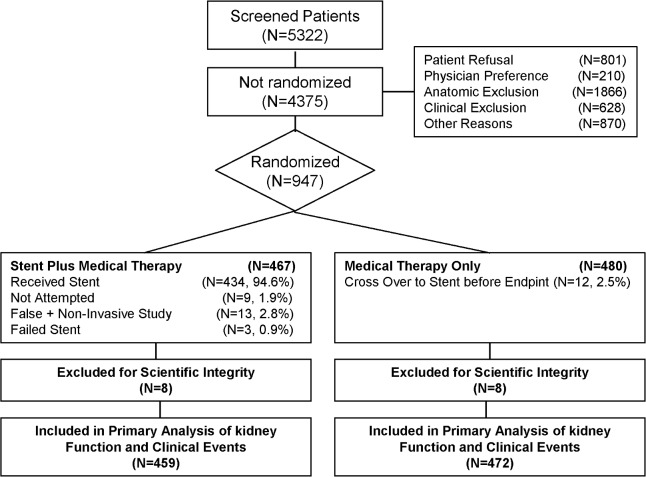
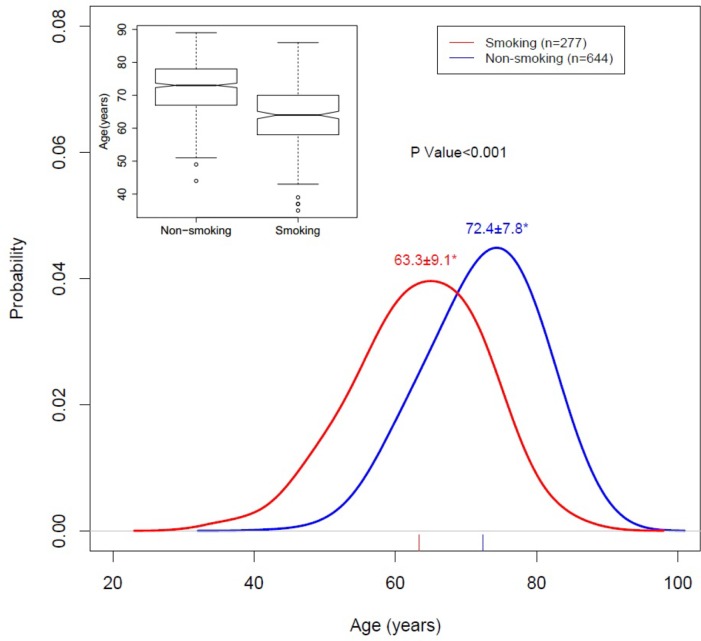
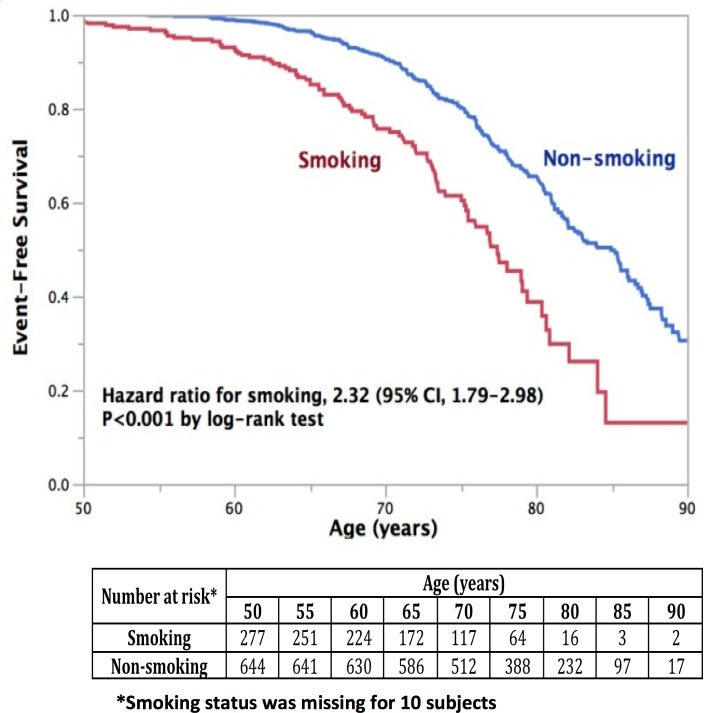
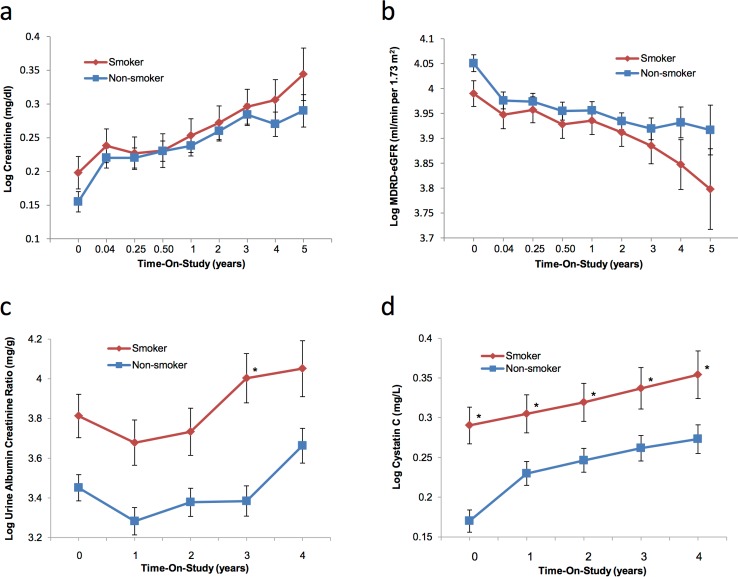
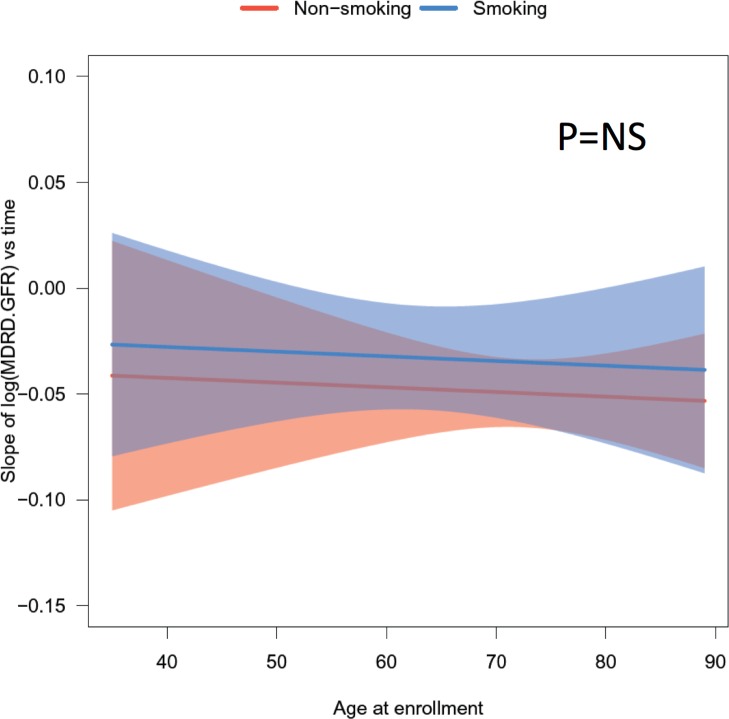
Cigarette smoking causes cardiovascular disease and is associated with poor kidney function in individuals with diabetes mellitus and primary kidney diseases. However, the association of smoking on patients with atherosclerotic renal artery stenosis has not been studied. The current study utilized data from the Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL, NCT00081731) clinical trial to evaluate the effects of smoking on the risk of cardio-renal events and kidney function in this population. Baseline data showed that smokers (n = 277 out of 931) were significantly younger at enrollment than non-smokers (63.3±9.1 years vs 72.4±7.8 years; p<0.001). In addition, patients who smoke were also more likely to have bilateral renal artery stenoses and peripheral vascular disease (PVD). Longitudinal analysis showed that smokers experienced composite endpoint events (defined as first occurrence of: stroke; cardiovascular or renal death; myocardial infarction; hospitalization for congestive heart failure; permanent renal replacement; and progressive renal insufficiency defined as 30% reduction of GFR from baseline sustained for ≥ 60 days) at a substantially younger age compared to non-smokers (67.1±9.0 versus 76.1±7.9, p<0.001). Using linear regression and generalized linear modeling analysis controlled by age, sex, and ethnicity, smokers had significantly higher cystatin C levels (1.3±0.7 vs 1.2±0.9, p<0.01) whereas creatinine and estimated glomerular filtration rate (eGFR) were not different from non-smokers. From these data we conclude that smoking has a significant association with deleterious cardio-renal outcomes in patients with renovascular hypertension.
Conflict of interest statement
Figures
Similar articles
-
Effects of Stenting for Atherosclerotic Renal Artery Stenosis on eGFR and Predictors of Clinical Events in the CORAL Trial.Clin J Am Soc Nephrol. 2016 Jul 7;11(7):1180-1188. doi: 10.2215/CJN.10491015. Epub 2016 May 25. Clin J Am Soc Nephrol. 2016. PMID: 27225988 Free PMC article. Clinical Trial.
-
A study on the outcome of percutaneous transluminal renal angioplasty in patients with renal failure.Nephron Clin Pract. 2006;104(3):c132-42. doi: 10.1159/000094916. Epub 2006 Aug 7. Nephron Clin Pract. 2006. PMID: 16899992
-
Stent revascularization for the prevention of cardiovascular and renal events among patients with renal artery stenosis and systolic hypertension: rationale and design of the CORAL trial.Am Heart J. 2006 Jul;152(1):59-66. doi: 10.1016/j.ahj.2005.09.011. Am Heart J. 2006. PMID: 16824832
-
Renal Artery Stenosis: New Findings from the CORAL Trial.Curr Cardiol Rep. 2017 Sep;19(9):75. doi: 10.1007/s11886-017-0894-2. Curr Cardiol Rep. 2017. PMID: 28752274 Review.
-
[Ischemic renal disease: revascularization or conservative treatment?].Nefrologia. 2005;25(3):258-68. Nefrologia. 2005. PMID: 16053007 Review. Spanish.
Cited by
-
Renovascular Hypertension.Endocrinol Metab Clin North Am. 2019 Dec;48(4):765-778. doi: 10.1016/j.ecl.2019.08.007. Epub 2019 Sep 19. Endocrinol Metab Clin North Am. 2019. PMID: 31655775 Free PMC article. Review.
-
Bilateral renal artery stenosis in a young man.BMJ Case Rep. 2021 Aug 13;14(8):e237608. doi: 10.1136/bcr-2020-237608. BMJ Case Rep. 2021. PMID: 34389585 Free PMC article.
-
Atherosclerotic Renovascular Disease: A KDIGO (Kidney Disease: Improving Global Outcomes) Controversies Conference.Am J Kidney Dis. 2022 Feb;79(2):289-301. doi: 10.1053/j.ajkd.2021.06.025. Epub 2021 Aug 9. Am J Kidney Dis. 2022. PMID: 34384806 Free PMC article.
-
Relationship between 24-h Ambulatory Blood Pressure Variability and Degree of Renal Artery Stenosis in Hospitalized Patients with Hypertension.Rev Cardiovasc Med. 2024 Nov 8;25(11):397. doi: 10.31083/j.rcm2511397. eCollection 2024 Nov. Rev Cardiovasc Med. 2024. PMID: 39618844 Free PMC article.
-
Blood Glucose and Renal Function Evaluation in Patients with Viral Hepatitis.Diabetes Metab Syndr Obes. 2021 Jul 20;14:3337-3344. doi: 10.2147/DMSO.S303252. eCollection 2021. Diabetes Metab Syndr Obes. 2021. PMID: 34321900 Free PMC article.
References
-
- Centers for Disease C, Prevention. Smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 2000–2004. MMWR Morbidity and mortality weekly report. 2008;57(45):1226–8. Epub 2008/11/15. - PubMed
-
- Orth SR. Smoking and the Kidney. Journal of the American Society of Nephrology. 2002;13(6):1663–72. - PubMed
MeSH terms
Grants and funding
- U01HL072735/NH/NIH HHS/United States
- 13POST16860035/American Heart Association/International
- R01-HL-105649/NH/NIH HHS/United States
- U01HL072737/NH/NIH HHS/United States
- F32DK104615-01/NH/NIH HHS/United States
- R01 HL105649/HL/NHLBI NIH HHS/United States
- U01 HL071556/HL/NHLBI NIH HHS/United States
- 5U01HL071556/NH/NIH HHS/United States
- R01 HL109015/HL/NHLBI NIH HHS/United States
- U01HL072736/NH/NIH HHS/United States
- R01-HL-109015/NH/NIH HHS/United States
- U01HL072734/NH/NIH HHS/United States
- F32 DK104615/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
