

Dysregulation of Alveolar Macrophage PPARγ, NADPH Oxidases, and TGFβ1 in Otherwise Healthy HIV-Infected Individuals
- PMID: 28314381
- PMCID: PMC5650722
- DOI: 10.1089/AID.2016.0030
Dysregulation of Alveolar Macrophage PPARγ, NADPH Oxidases, and TGFβ1 in Otherwise Healthy HIV-Infected Individuals
Abstract
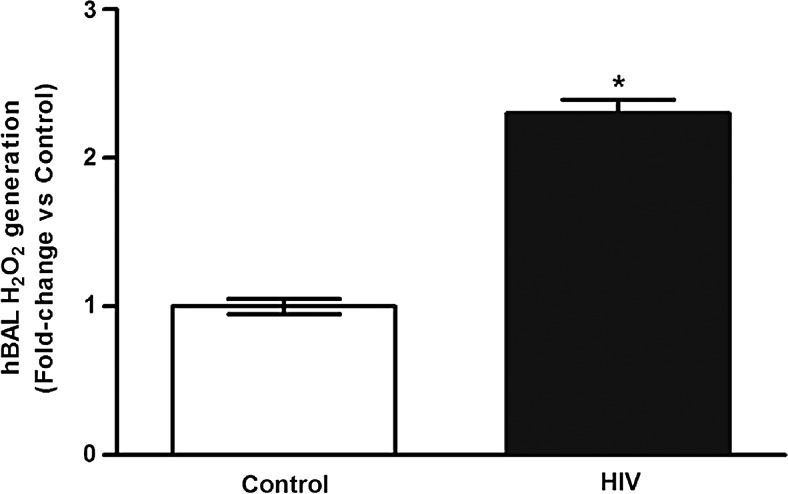
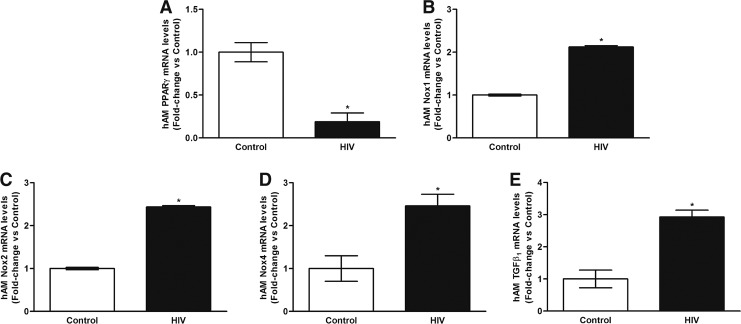
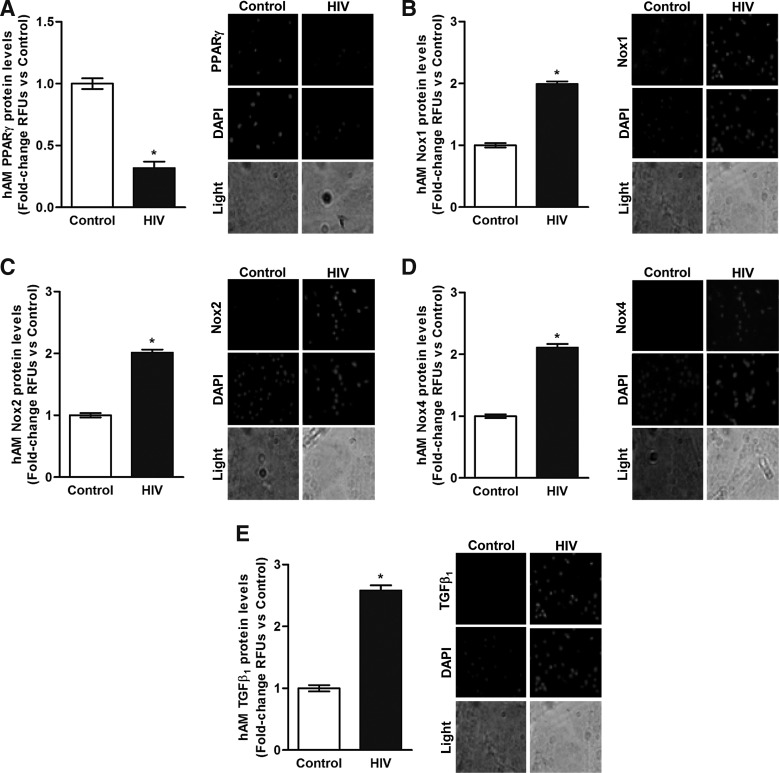
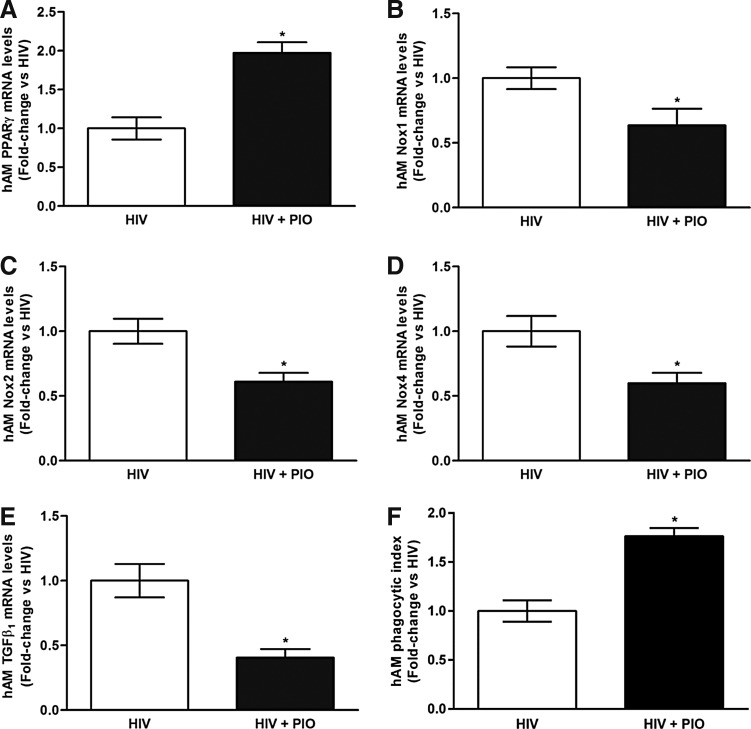
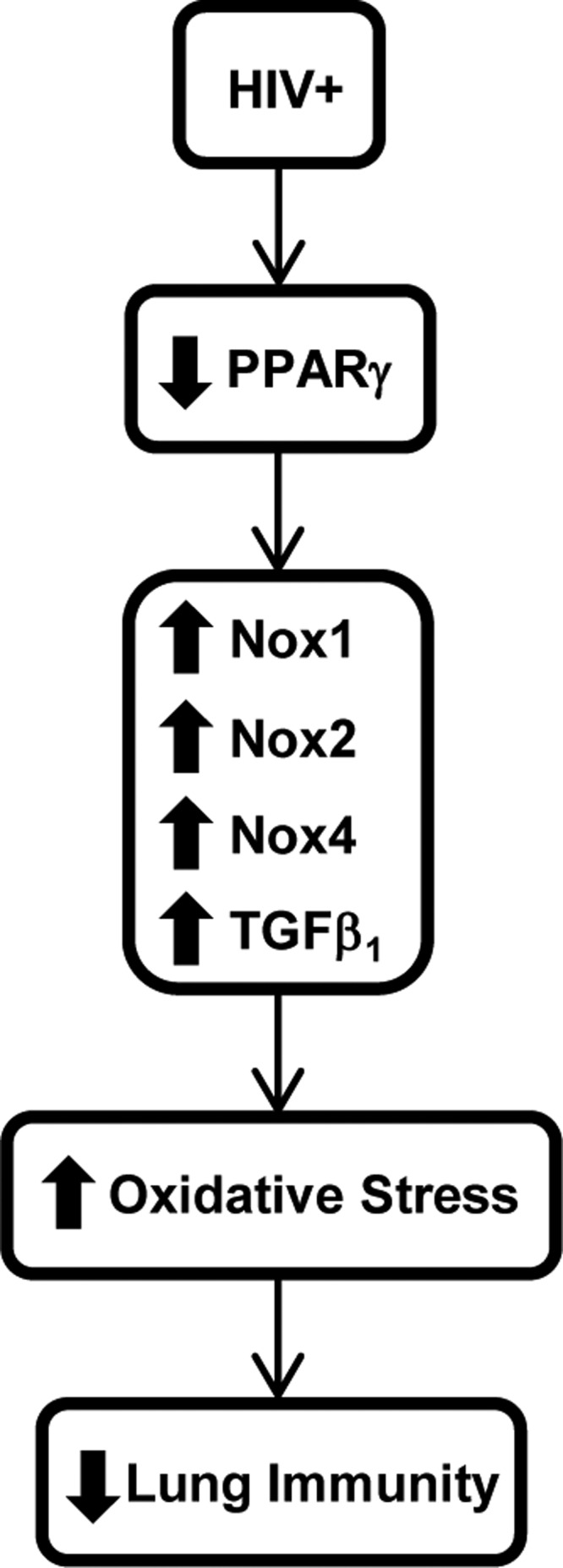
Despite antiretroviral therapy (ART), respiratory infections increase mortality in individuals living with chronic human immunodeficiency virus (HIV) infection. In experimental and clinical studies of chronic HIV infection, alveolar macrophages (AMs) exhibit impaired phagocytosis and bacterial clearance. Peroxisome proliferator-activated receptor (PPAR)γ, NADPH oxidase (Nox) isoforms Nox1, Nox2, Nox4, and transforming growth factor-beta 1 (TGFβ1) are critical mediators of AM oxidative stress and phagocytic dysfunction. Therefore, we hypothesized that HIV alters AM expression of these targets, resulting in chronic lung oxidative stress and subsequent immune dysfunction. A cross-sectional study of HIV-infected (n = 22) and HIV-uninfected (n = 6) subjects was conducted. Bronchoalveolar lavage (BAL) was performed, and AMs were isolated. Lung H2O2 generation was determined by measuring H2O2 in the BAL fluid. In AMs, PPARγ, Nox1, Nox2, Nox4, and TGFβ1 mRNA (quantitative real-time polymerase chain reaction) and protein (fluorescent immunomicroscopy) levels were assessed. Compared with HIV-uninfected (control) subjects, HIV-infected subjects were relatively older and the majority were African American; ∼86% were on ART, and their median CD4 count was 445, with a median viral load of 0 log copies/ml. HIV infection was associated with increased H2O2 in the BAL, decreased AM mRNA and protein levels of PPARγ, and increased AM mRNA and protein levels of Nox1, Nox2, Nox4, and TGFβ1. PPARγ attenuation and increases in Nox1, Nox2, Nox4, and TGFβ1 contribute to AM oxidative stress and immune dysfunction in the AMs of otherwise healthy HIV-infected subjects. These findings provide novel insights into the molecular mechanisms by which HIV increases susceptibility to pulmonary infections.
Keywords: HIV; immunology; molecular biology.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Li TS, Tubiana R, Katlama C, Calvez V, Ait Mohand H, Autran B: Long-lasting recovery in CD4 T-cell function and viral-load reduction after highly active antiretroviral therapy in advanced HIV-1 disease. Lancet 1998;351:1682–1686 - PubMed
-
- Mellors JW, Munoz A, Giorgi JV, Margolick JB, Tassoni CJ, Gupta P, et al. : Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med 1997;126:946–954 - PubMed
-
- Jordano Q, Falco V, Almirante B, Planes AM, del Valle O, Ribera E, et al. : Invasive pneumococcal disease in patients infected with HIV: Still a threat in the era of highly active antiretroviral therapy. Clin Infect Dis 2004;38:1623–1628 - PubMed
-
- Strategies for Management of Antiretroviral Therapy Study Group; El-Sadr WM, Lundgren J, Neaton JD, Gordin F, Abrams D, et al. : CD4+ count-guided interruption of antiretroviral treatment. N Engl J Med 2006;355:2283–2296 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
