

Cerebral microhemorrhages: mechanisms, consequences, and prevention
- PMID: 28314762
- PMCID: PMC5495931
- DOI: 10.1152/ajpheart.00780.2016
Cerebral microhemorrhages: mechanisms, consequences, and prevention
Abstract
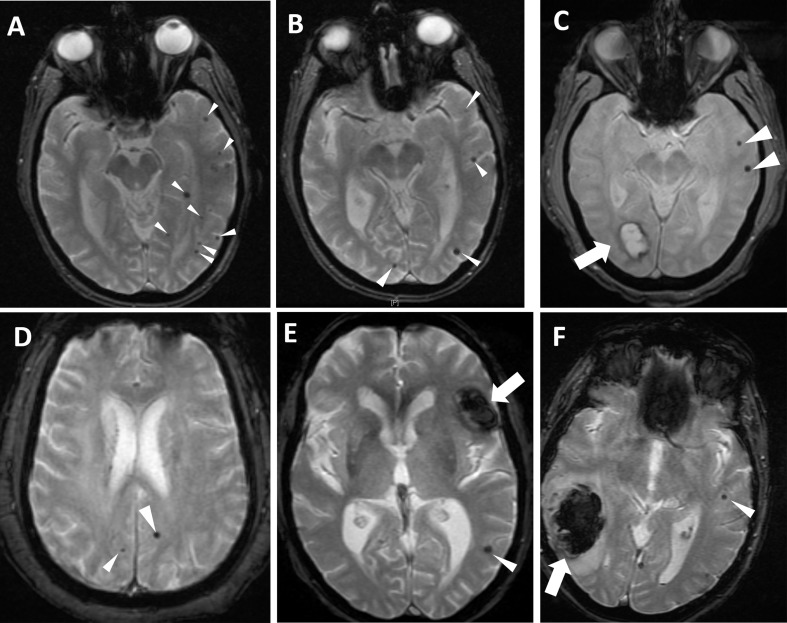
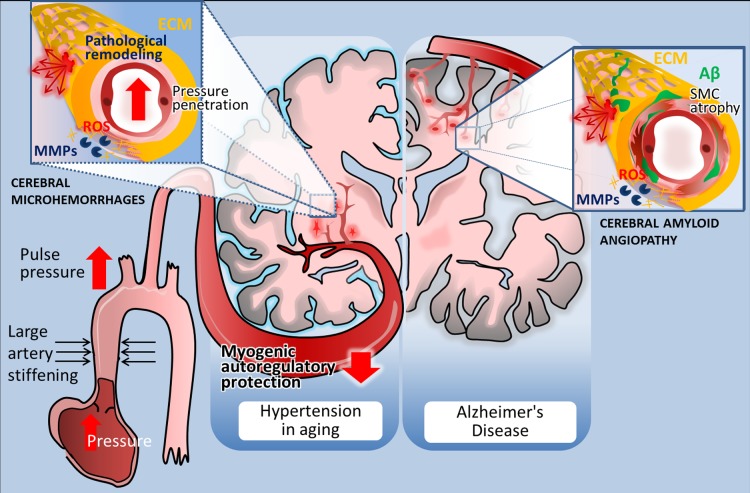
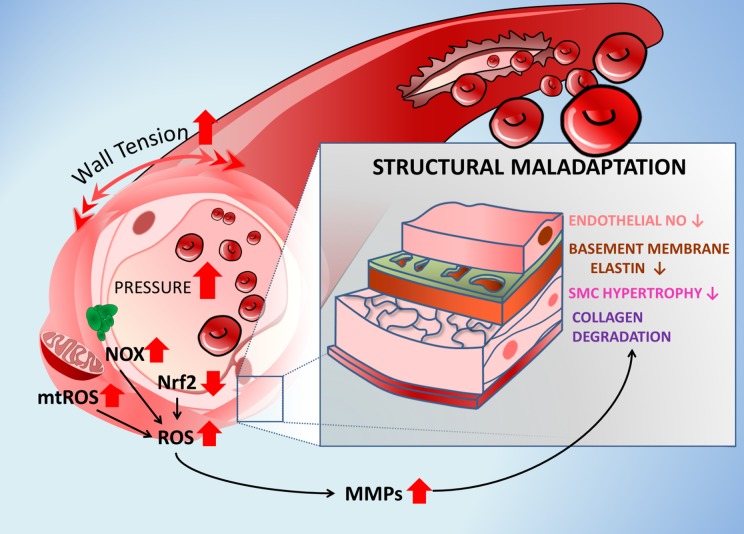
The increasing prevalence of multifocal cerebral microhemorrhages (CMHs, also known as "cerebral microbleeds") is a significant, newly recognized problem in the aging population of the Western world. CMHs are associated with rupture of small intracerebral vessels and are thought to progressively impair neuronal function, potentially contributing to cognitive decline, geriatric psychiatric syndromes, and gait disorders. Clinical studies show that aging and hypertension significantly increase prevalence of CMHs. CMHs are also now recognized by the National Institutes of Health as a major factor in Alzheimer's disease pathology. Moreover, the presence of CMHs is an independent risk factor for subsequent larger intracerebral hemorrhages. In this article, we review the epidemiology, detection, risk factors, clinical significance, and pathogenesis of CMHs. The potential age-related cellular mechanisms underlying the development of CMHs are discussed, with a focus on the structural determinants of microvascular fragility, age-related alterations in cerebrovascular adaptation to hypertension, the role of oxidative stress and matrix metalloproteinase activation, and the deleterious effects of arterial stiffening, increased pulse pressure, and impaired myogenic autoregulatory protection on the brain microvasculature. Finally, we examine potential treatments for the prevention of CMHs based on the proposed model of aging- and hypertension-dependent activation of the reactive oxygen species-matrix metalloproteinases axis, and we discuss critical questions to be addressed by future studies.
Keywords: cerebromicrovascular; cerebrovascular; stroke; transient ischemic attack; vascular aging; vascular cognitive impairment; vascular contributors to cognitive impairment and dementia.
Figures
References
-
- Arboleda-Velasquez JF, Manent J, Lee JH, Tikka S, Ospina C, Vanderburg CR, Frosch MP, Rodríguez-Falcón M, Villen J, Gygi S, Lopera F, Kalimo H, Moskowitz MA, Ayata C, Louvi A, Artavanis-Tsakonas S. Hypomorphic Notch 3 alleles link Notch signaling to ischemic cerebral small-vessel disease. Proc Natl Acad Sci USA 108: E128–E135, 2011. doi: 10.1073/pnas.1101964108. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources