

Review
doi: 10.1161/JAHA.117.005543.
Coronary Atherosclerotic Vulnerable Plaque: Current Perspectives
Affiliations
- PMID: 28314799
- PMCID: PMC5524044
- DOI: 10.1161/JAHA.117.005543
Item in Clipboard
Review
Coronary Atherosclerotic Vulnerable Plaque: Current Perspectives
J Am Heart Assoc.
.
No abstract available
Keywords: atherogenesis; treatment; vulnerable plaque.
Figures
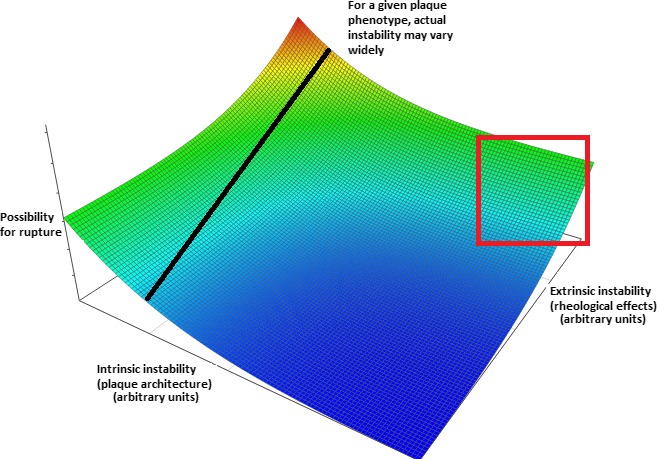
Inadequacy of modern approaches to detect plaque vulnerability. Conceptual plot visualizing the combined effects of factors leading to intrinsic and extrinsic plaque instability. Arbitrary “instability units” are used and the precise form of the relationship is purely conjectural—however, it was chosen to denote the more‐than‐additive effect of simultaneous increases in both parameters. The line drawn corresponds to plaques with a specific internal architecture and demonstrates that their actual instability (ie, possibility for rupture) is also critically dependent on external stresses applied to them. Of note, solely intrinsic features may indeed determine a truly destabilization‐prone plaque, but only at extreme values (thus clinically yielding high specificity and low sensitivity as potential criteria). Furthermore, imaging modalities rarely assess all features of vulnerability (in the current sense)—rather, they focus on specific aspects, such as lipid and calcium content, thus failing in even establishing the value in the intrinsic instability axis. Moreover, both these parameters vary with time given the (1) tendency of plaques to alternate between different structural phenotypes and (2) possibility for alterations in the rheological (dynamic pressure, pressure head, and viscosity) features of circulation (eg, following removal of an upstream lesion through successful angioplasty)—thus, a given plaque's position would not remain fixed on the plot. Clustering could be anticipated to occur in several areas of the plot, given that, often, intrinsic features affect extrinsic and vice versa (ie, a thick‐capped fibrous occlusive plaque would be subject to higher external stresses and thus usually be located in the area enclosed by the red square). Models incorporating all mentioned aspects would likely yield a much more accurate prediction regarding possibility for rupture and (should further parameters such as viscosity be added) acute events (even if silent) and thus guide treatment. Color coding: blue, red: minimal and maximal instability, respectively.
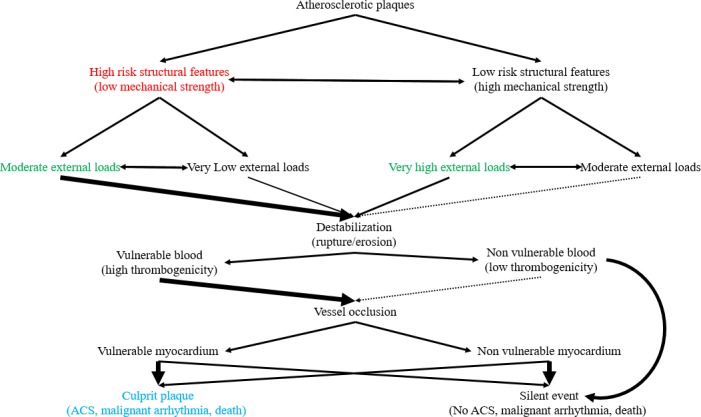
Projected natural course of atherosclerotic plaques based on their intrinsic and extrinsic features. This figure depicts potential evolution of plaques based on an integrative assessment, including external and internal factors, and underlies the necessary paradigm shift in the vulnerable plaque definition. Size and thickness of arrows implies relative probability for a course between the 2 listed in every step. Obviously, the default state, that is, maintenance of the status quo with plaques remaining quiescent, is far more likely in all cases—no arrow denotes certainty for an event. As seen in the diagram, even stable, by all accounts, plaques can rupture/erode. This can be attributed to a phenotype/external stressor shift, an erroneous assessment, or simply an unlikely event given that plaque behavior is, as everything in medicine, the sum of probabilistic, not determinate, events. Additional levels of uncertainty are inserted through the, currently unpredictable, blood and myocardium response to a destabilizing event. Nonvulnerable blood and plaque destabilization combination may also lead to events, albeit rarely. “Silent” events are considered, for the purposes of this figure, both those resolving previous to thrombus formation and those with thrombosis yet remaining clinically undetected. “High” and “low” risk structural features can only be defined relatively, that is, how would the plaque behave in cases of applied loads that can be considered moderate. Obviously, further research is necessary to elucidate these parameters. Color coding: blue—initial definition; red—current perception; green—integrative approach. Double‐headed arrows denote bidirectional processes. ACS indicates acute coronary syndrome.
References
-
- WHO . Cardiovascular diseases (CVDs). Fact sheet ‐ Reviewed June. 2016.
-
- Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, Badimon JJ, Stefanadis C, Moreno P, Pasterkamp G, Fayad Z, Stone PH, Waxman S, Raggi P, Madjid M, Zarrabi A, Burke A, Yuan C, Fitzgerald PJ, Siscovick DS, de Korte CL, Aikawa M, Airaksinen KE, Assmann G, Becker CR, Chesebro JH, Farb A, Galis ZS, Jackson C, Jang IK, Koenig W, Lodder RA, March K, Demirovic J, Navab M, Priori SG, Rekhter MD, Bahr R, Grundy SM, Mehran R, Colombo A, Boerwinkle E, Ballantyne C, Insull W Jr, Schwartz RS, Vogel R, Serruys PW, Hansson GK, Faxon DP, Kaul S, Drexler H, Greenland P, Muller JE, Virmani R, Ridker PM, Zipes DP, Shah PK, Willerson JT. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part II. Circulation. 2003;108:1772–1778. - PubMed
-
- Naghavi M, Libby P, Falk E, Casscells SW, Litovsky S, Rumberger J, Badimon JJ, Stefanadis C, Moreno P, Pasterkamp G, Fayad Z, Stone PH, Waxman S, Raggi P, Madjid M, Zarrabi A, Burke A, Yuan C, Fitzgerald PJ, Siscovick DS, de Korte CL, Aikawa M, Juhani Airaksinen KE, Assmann G, Becker CR, Chesebro JH, Farb A, Galis ZS, Jackson C, Jang IK, Koenig W, Lodder RA, March K, Demirovic J, Navab M, Priori SG, Rekhter MD, Bahr R, Grundy SM, Mehran R, Colombo A, Boerwinkle E, Ballantyne C, Insull W Jr, Schwartz RS, Vogel R, Serruys PW, Hansson GK, Faxon DP, Kaul S, Drexler H, Greenland P, Muller JE, Virmani R, Ridker PM, Zipes DP, Shah PK, Willerson JT. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: Part I. Circulation. 2003;108:1664–1672. - PubMed
-
- Bourantas CV, Garcia‐Garcia HM, Farooq V, Maehara A, Xu K, Genereux P, Diletti R, Muramatsu T, Fahy M, Weisz G, Stone GW, Serruys PW. Clinical and angiographic characteristics of patients likely to have vulnerable plaques: analysis from the PROSPECT study. JACC Cardiovasc Imaging. 2013;6:1263–1272. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
