

Editorial
doi: 10.1136/bjophthalmol-2016-309764.
Epub 2017 Mar 17.
Why birdshot retinochoroiditis should rather be called 'HLA-A29 uveitis'?
Affiliations
- PMID: 28314830
- PMCID: PMC5530806
- DOI: 10.1136/bjophthalmol-2016-309764
Item in Clipboard
Editorial
Why birdshot retinochoroiditis should rather be called 'HLA-A29 uveitis'?
Br J Ophthalmol.
2017 Jul.
No abstract available
Keywords: Choroid; Immunology; Inflammation; Retina.
Conflict of interest statement
Competing interests: None declared.
Figures
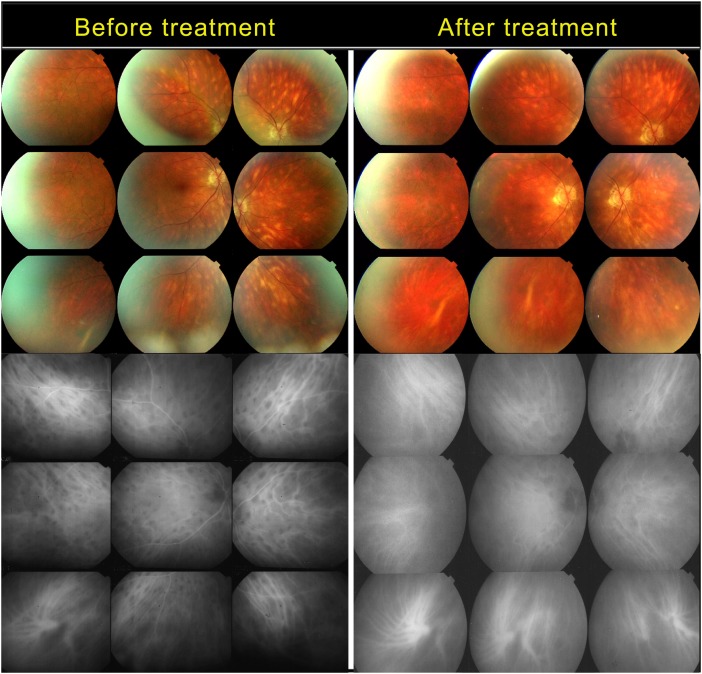
Birdshot fundus lesions (BFLs) do not correspond to hypofluorescent dark dots (HDDs). Case of birdshot retinochoroiditis that lasted for >5 years before the patient agreed to treatment. Top left: untreated patient; many BFLs are present in the fundus. Bottom left, indocyanine green angiography (ICGA) frame, the presence of numerous HDDs indicating active disease; however, there are more angiographically silent BFLs than HDDs. Top right: the fundus after 7 years of treatment with persisting BFLs. Bottom right: ICGA frame showing that neither resolved HDDs nor BFLs appear on ICGA (angiographically silent).
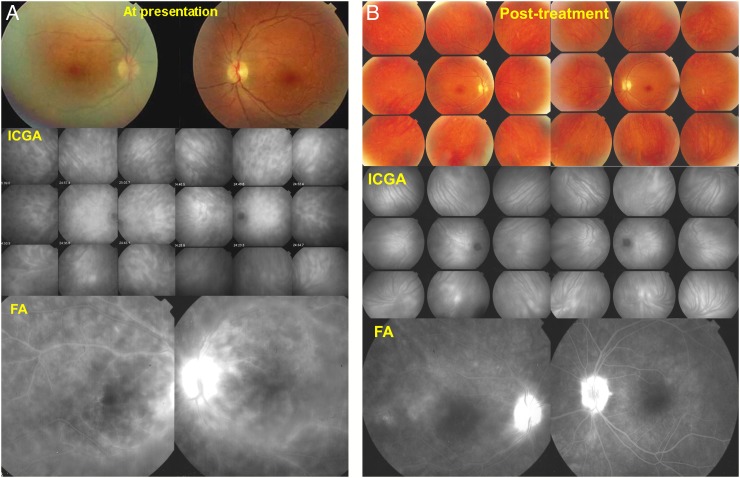
(A) Case of birdshot retinochoroiditis diagnosed before birdshot fundus lesions (BFLs) were visible. Top: fundus pictures of the right and left eye. No BFLs seen. Middle: indocyanine green angiography (ICGA) showing numerous HDDs on both sides. Bottom: diffuse retinal vasculitis involving veins of all sizes with diffuse leakage. (B) Same case as (A) after 10 years of immunosuppressive therapy. Top: fundus pictures of right and left eye showing absence of typical BFLs. Middle: ICGA shows a totally normal choroid indicating that the choroid is responding easily to immunosuppressive therapy with resolution of all lesions. Bottom: fluorescein angiography (FA) shows that retinal vasculitis is substantially improved; however, discreet leakage is still present, and there is bilateral disc hyperfluorescence.
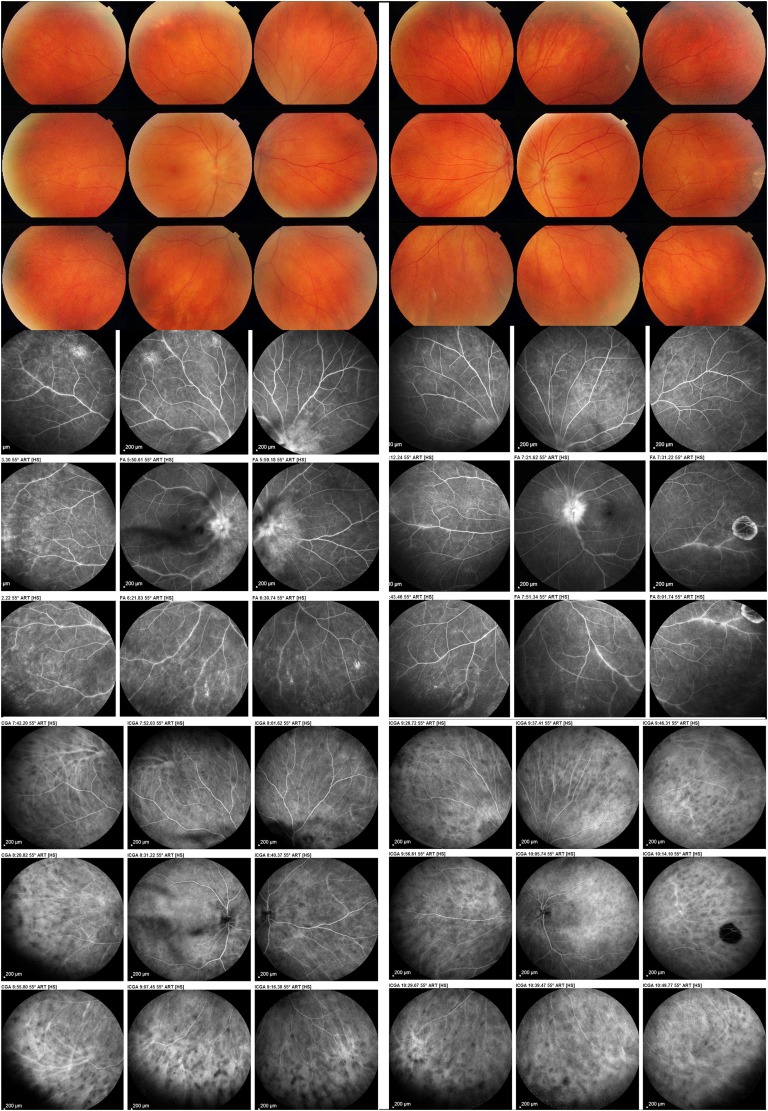
Case of birdshot retinochoroiditis without birdshot fundus lesions at presentation. The patient was referred for retinal vasculitis and also complained of floaters bilaterally. Posterior segment showed numerous vitreous opacities but no fundus lesions (top). Middle: diffuse retinal vasculitis in both eyes. Bottom: typical indocyanine green angiography signs of stromal choroiditis with numerous HDDs and non-recognizable pattern of choroidal vessels. The patient was immediately tested for the presence of HLA-A29 antigen, which was indeed positive.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials