

Exercise-Associated Hyponatremia: 2017 Update
- PMID: 28316971
- PMCID: PMC5334560
- DOI: 10.3389/fmed.2017.00021
Exercise-Associated Hyponatremia: 2017 Update
Abstract
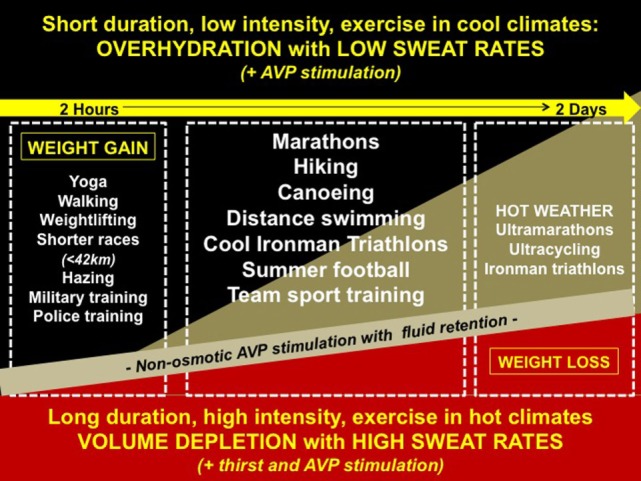
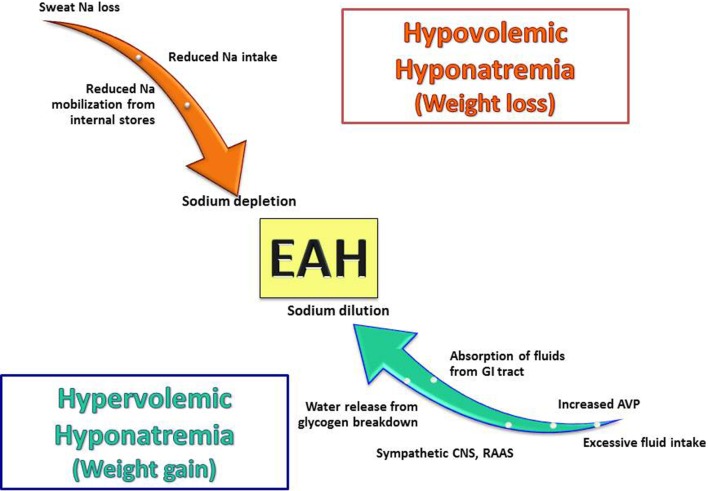
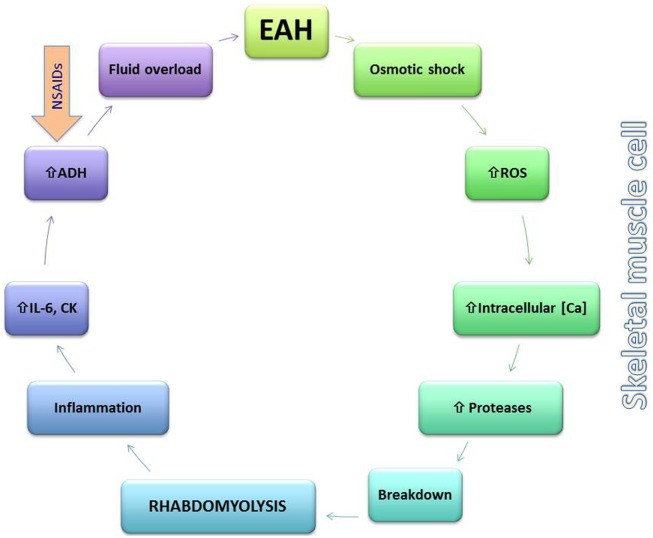
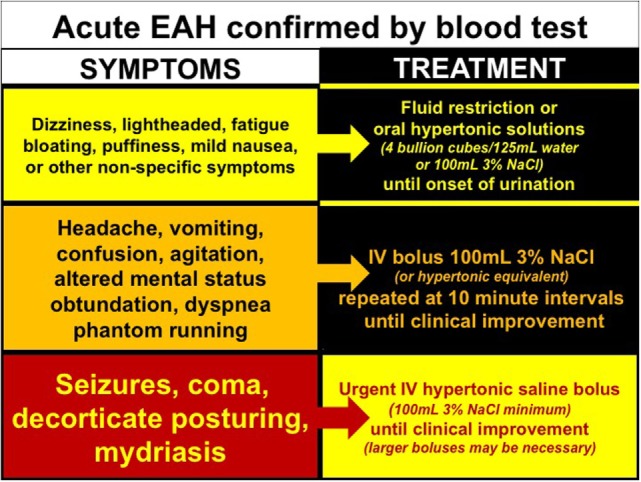
Exercise-associated hyponatremia (EAH) was initially described in the 1980s in endurance athletes, and work done since then has conclusively identified that overdrinking beyond thirst and non-osmotic arginine vasopressin release are the most common etiologic factors. In recent years, EAH has been described in a broader variety of athletic events and also has been linked to the development of rhabdomyolysis. The potential role of volume and sodium depletion in a subset of athletes has also been described. This review focuses on the most recent literature in the field of EAH and summarizes key new findings in the epidemiology, pathophysiology, treatment, and prevention of this condition.
Keywords: exercise; hyponatremia; pathogenesis; rhabdomyolysis; water.
Figures
References
-
- Jones BL, O’Hara JP, Till K, King RF. Dehydration and hyponatremia in professional rugby union players: a cohort study observing English premiership rugby union players during match play, field, and gym training in cool environmental conditions. J Strength Cond Res (2015) 29(1):107–15. 10.1519/JSC.0000000000000620 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources