

Vitiligo Pathogenesis and Emerging Treatments
- PMID: 28317534
- PMCID: PMC5362109
- DOI: 10.1016/j.det.2016.11.014
Vitiligo Pathogenesis and Emerging Treatments
Abstract
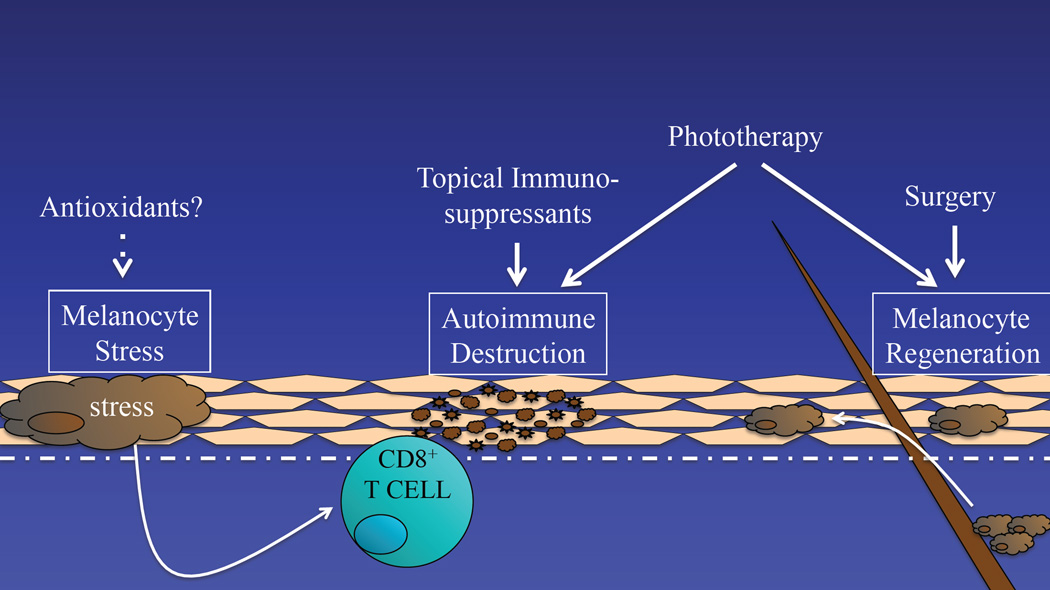
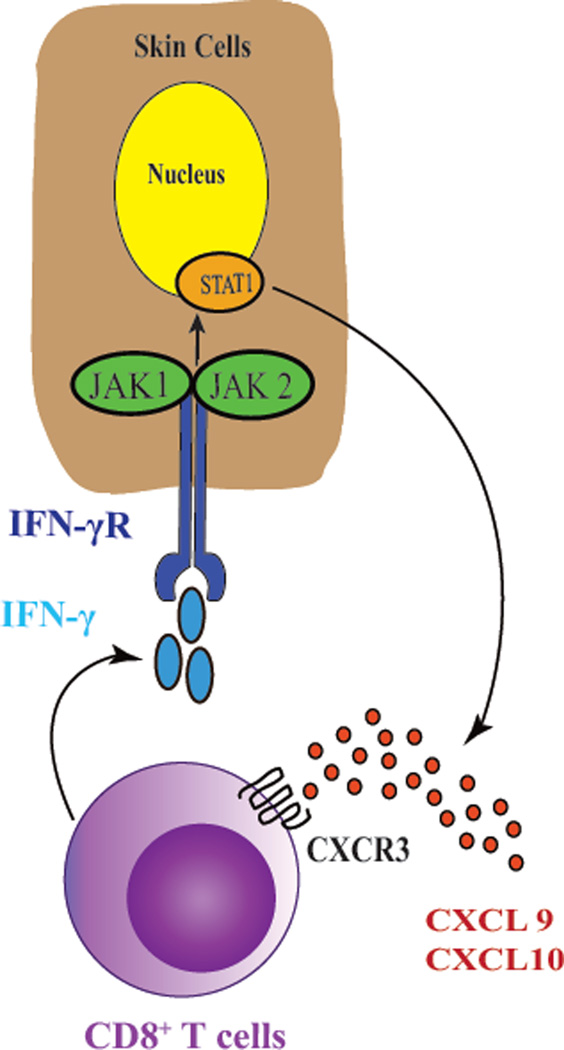
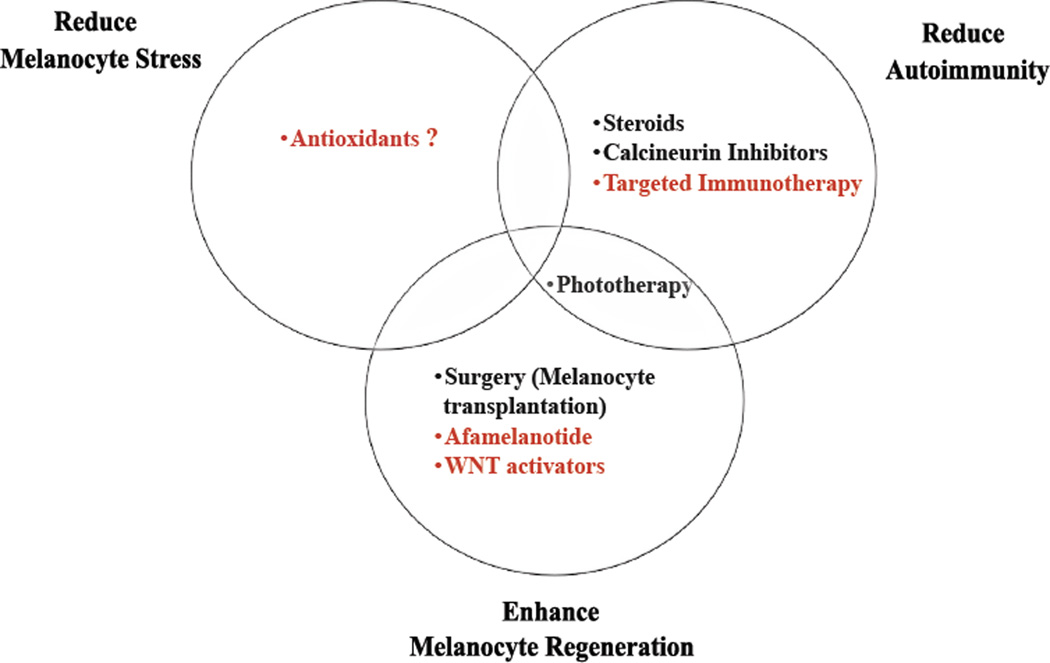
The pathogenesis of vitiligo involves interplay between intrinsic and extrinsic melanocyte defects, innate immune inflammation, and T-cell-mediated melanocyte destruction. The goal of treatment is to not only halt disease progression but also promote repigmentation through melanocyte regeneration, proliferation, and migration. Treatment strategies that address all aspects of disease pathogenesis and repigmentation are likely to have greatest efficacy, a strategy that may require combination therapies. Current treatments generally involve nontargeted suppression of autoimmunity, whereas emerging treatments are likely to use a more targeted approach based on in-depth understanding of disease pathogenesis, which may provide higher efficacy with a good safety profile.
Keywords: Autoimmunity; Cellular stress; Chemokines; Melanogenesis; Targeted therapy; Vitiligo.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Ezzedine K, Eleftheriadou V, Whitton M, van Geel N. Vitiligo. Lancet. 2015;386(9988):74–84. - PubMed
-
- Dell'Anna MLEK, Hamzavi I, Harris J, Parsad D, Taieb A, Picardo M. Vitiligo. Nature Reviews Disease Primers. 2015;1(1):1–16. - PubMed
-
- Taieb A, Picardo M. Clinical practice. Vitiligo. N Engl J Med. 2009;360(2):160–169. - PubMed
-
- Alkhateeb A, Fain PR, Thody A, Bennett DC, Spritz RA. Epidemiology of vitiligo and associated autoimmune diseases in Caucasian probands and their families. Pigment Cell Res. 2003;16(3):208–214. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
