

Editorial
doi: 10.1200/JCO.2017.72.2660.
Epub 2017 Mar 20.
Effects of Smoking on Late Toxicity From Breast Radiation
Affiliations
- PMID: 28319432
- PMCID: PMC5890437
- DOI: 10.1200/JCO.2017.72.2660
Item in Clipboard
Editorial
Effects of Smoking on Late Toxicity From Breast Radiation
J Clin Oncol.
.
No abstract available
Figures
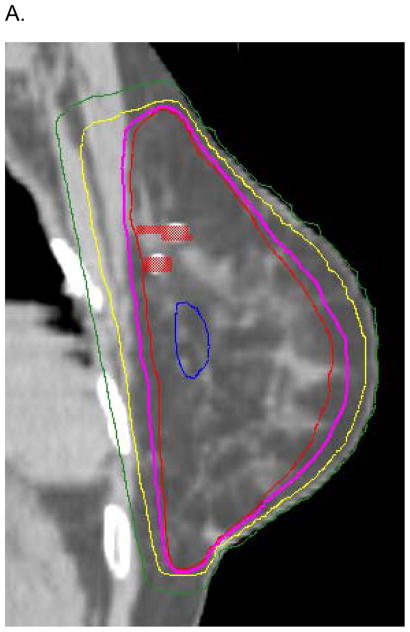
This is a 44 year old woman with a 27 pack-year smoking history who presented with a pT1c N0 (i+, sn) invasive ductal carcinoma of the upper outer quadrant of the left breast, intermediate grade, ER+, PR+, HER2−. She underwent margin-negative breast conserving surgery with sentinel node biopsy. Oncotype DX score was 9. She was treated with 40 Gy in 15 fractions in the prone position followed by a 10 Gy in 5 fraction boost in the lateral decubitus position. Prone positioning with judicious tangent beam placement was utilized to achieve a mean heart dose of 0.6 Gy and a mean total lung dose of 0.2 Gy. A – parasagittal slice of the radiation treatment plan, B – axial slice of radiation treatment plan. Tumor bed clips are show in red. Isodose lines are as follows: 106% - blue; 100% - red; 98% - purple; 90% - yellow; 50% - green.

This is a 44 year old woman with a 27 pack-year smoking history who presented with a pT1c N0 (i+, sn) invasive ductal carcinoma of the upper outer quadrant of the left breast, intermediate grade, ER+, PR+, HER2−. She underwent margin-negative breast conserving surgery with sentinel node biopsy. Oncotype DX score was 9. She was treated with 40 Gy in 15 fractions in the prone position followed by a 10 Gy in 5 fraction boost in the lateral decubitus position. Prone positioning with judicious tangent beam placement was utilized to achieve a mean heart dose of 0.6 Gy and a mean total lung dose of 0.2 Gy. A – parasagittal slice of the radiation treatment plan, B – axial slice of radiation treatment plan. Tumor bed clips are show in red. Isodose lines are as follows: 106% - blue; 100% - red; 98% - purple; 90% - yellow; 50% - green.
Comment on
-
Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials.J Clin Oncol. 2017 May 20;35(15):1641-1649. doi: 10.1200/JCO.2016.72.0722. Epub 2017 Mar 20. J Clin Oncol. 2017. PMID: 28319436 Free PMC article.
References
-
- Moran MS, Schnitt SJ, Giuliano AE, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer. J Clin Oncol. 2014;32:1507–15. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–41. - PubMed
-
- Liu FF, Shi W, Done SJ, et al. Identification of a Low-Risk Luminal A Breast Cancer Cohort That May Not Benefit From Breast Radiotherapy. J Clin Oncol. 2015;33:2035–40. - PubMed
-
-
Taylor C. placeholder.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
