

Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials
- PMID: 28319436
- PMCID: PMC5548226
- DOI: 10.1200/JCO.2016.72.0722
Estimating the Risks of Breast Cancer Radiotherapy: Evidence From Modern Radiation Doses to the Lungs and Heart and From Previous Randomized Trials
Abstract
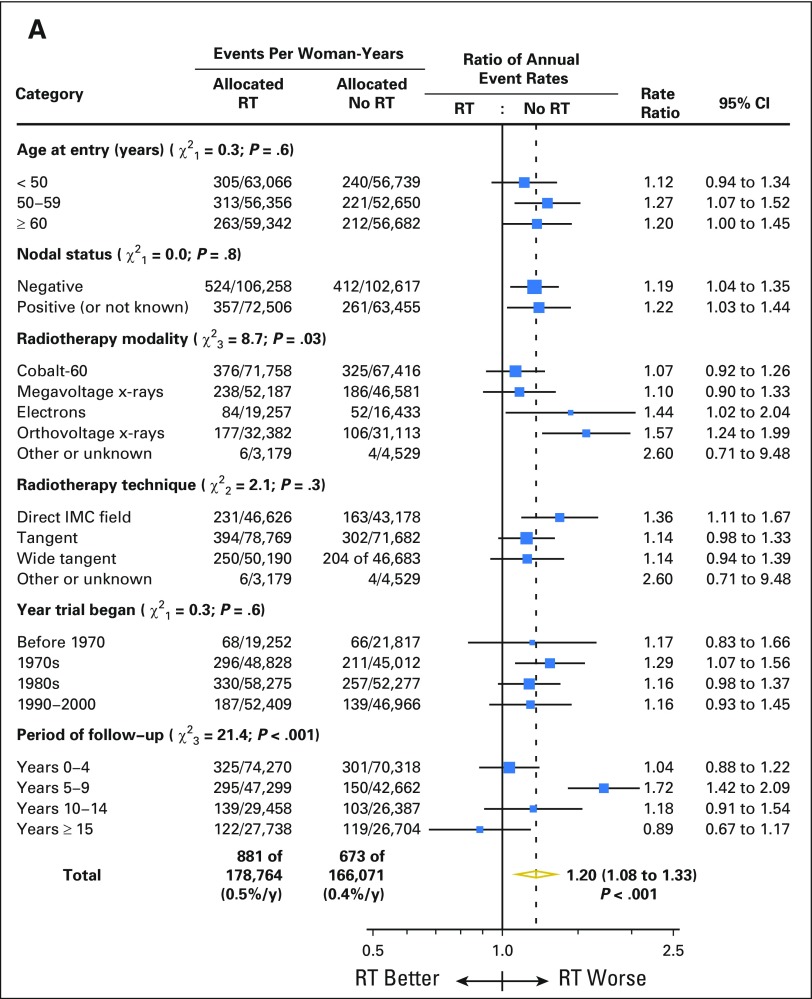
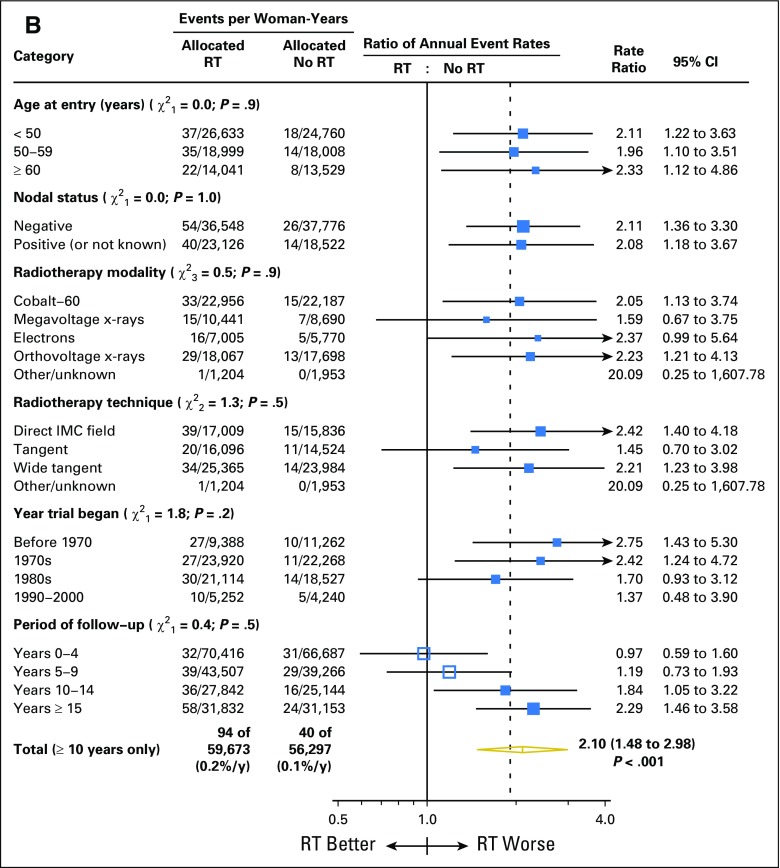
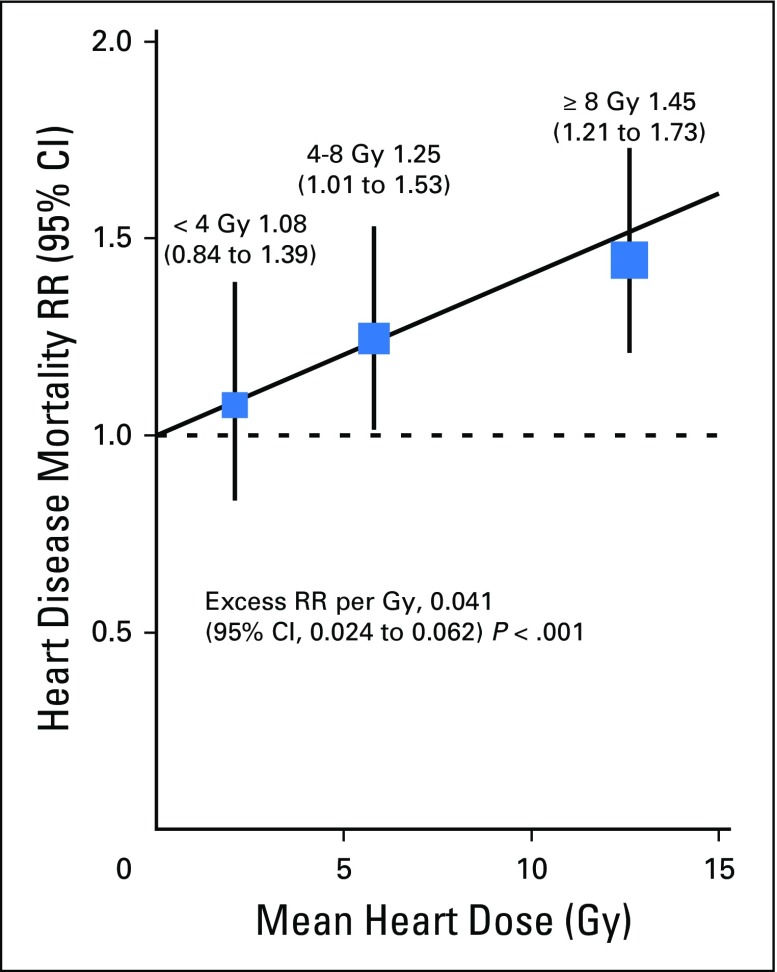
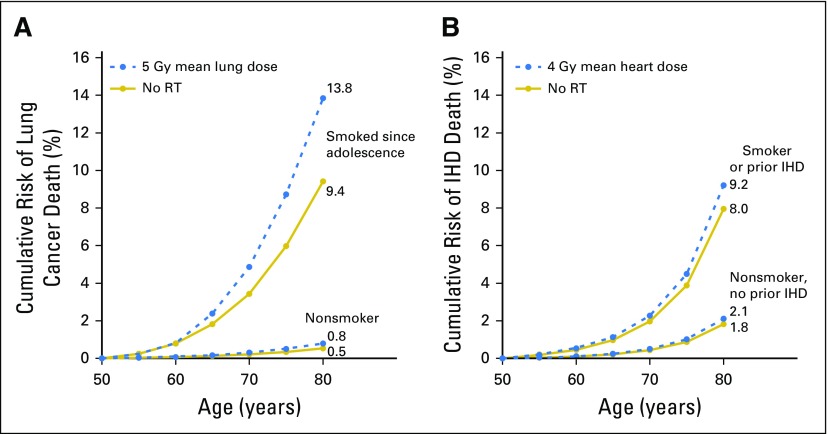
Purpose Radiotherapy reduces the absolute risk of breast cancer mortality by a few percentage points in suitable women but can cause a second cancer or heart disease decades later. We estimated the absolute long-term risks of modern breast cancer radiotherapy. Methods First, a systematic literature review was performed of lung and heart doses in breast cancer regimens published during 2010 to 2015. Second, individual patient data meta-analyses of 40,781 women randomly assigned to breast cancer radiotherapy versus no radiotherapy in 75 trials yielded rate ratios (RRs) for second primary cancers and cause-specific mortality and excess RRs (ERRs) per Gy for incident lung cancer and cardiac mortality. Smoking status was unavailable. Third, the lung or heart ERRs per Gy in the trials and the 2010 to 2015 doses were combined and applied to current smoker and nonsmoker lung cancer and cardiac mortality rates in population-based data. Results Average doses from 647 regimens published during 2010 to 2015 were 5.7 Gy for whole lung and 4.4 Gy for whole heart. The median year of irradiation was 2010 (interquartile range [IQR], 2008 to 2011). Meta-analyses yielded lung cancer incidence ≥ 10 years after radiotherapy RR of 2.10 (95% CI, 1.48 to 2.98; P < .001) on the basis of 134 cancers, indicating 0.11 (95% CI, 0.05 to 0.20) ERR per Gy whole-lung dose. For cardiac mortality, RR was 1.30 (95% CI, 1.15 to 1.46; P < .001) on the basis of 1,253 cardiac deaths. Detailed analyses indicated 0.04 (95% CI, 0.02 to 0.06) ERR per Gy whole-heart dose. Estimated absolute risks from modern radiotherapy were as follows: lung cancer, approximately 4% for long-term continuing smokers and 0.3% for nonsmokers; and cardiac mortality, approximately 1% for smokers and 0.3% for nonsmokers. Conclusion For long-term smokers, the absolute risks of modern radiotherapy may outweigh the benefits, yet for most nonsmokers (and ex-smokers), the benefits of radiotherapy far outweigh the risks. Hence, smoking can determine the net effect of radiotherapy on mortality, but smoking cessation substantially reduces radiotherapy risk.
Figures
Comment in
-
Effects of Smoking on Late Toxicity From Breast Radiation.J Clin Oncol. 2017 May 20;35(15):1633-1635. doi: 10.1200/JCO.2017.72.2660. Epub 2017 Mar 20. J Clin Oncol. 2017. PMID: 28319432 Free PMC article. No abstract available.
-
Cardiac Morbidity and Radiation Therapy for Breast Cancer.Int J Radiat Oncol Biol Phys. 2018 Feb 1;100(2):283-286. doi: 10.1016/j.ijrobp.2017.06.2443. Int J Radiat Oncol Biol Phys. 2018. PMID: 29353643 No abstract available.
-
[Estimating the long-term risks of breast cancer radiotherapy: evidence for lungs and heart].Strahlenther Onkol. 2018 Jul;194(7):693-694. doi: 10.1007/s00066-018-1310-6. Strahlenther Onkol. 2018. PMID: 29740663 German. No abstract available.
References
-
- Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;366:2087–2106. - PubMed
-
- Poortmans PM, Collette S, Kirkove C, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med. 2015;373:317–327. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
