

Hospital Characteristics Associated With Risk-standardized Readmission Rates
- PMID: 28319580
- PMCID: PMC5426655
- DOI: 10.1097/MLR.0000000000000713
Hospital Characteristics Associated With Risk-standardized Readmission Rates
Abstract
Background: Safety-net and teaching hospitals are somewhat more likely to be penalized for excess readmissions, but the association of other hospital characteristics with readmission rates is uncertain and may have relevance for hospital-centered interventions.
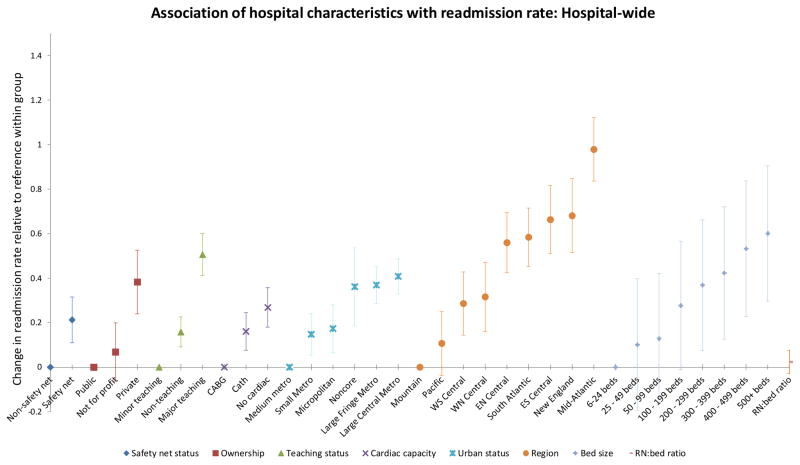
Objective: To examine the independent association of 8 hospital characteristics with hospital-wide 30-day risk-standardized readmission rate (RSRR).
Design: This is a retrospective cross-sectional multivariable analysis.
Subjects: US hospitals.
Measures: Centers for Medicare and Medicaid Services specification of hospital-wide RSRR from July 1, 2013 through June 30, 2014 with race and Medicaid dual-eligibility added.
Results: We included 6,789,839 admissions to 4474 hospitals of Medicare fee-for-service beneficiaries aged over 64 years. In multivariable analyses, there was regional variation: hospitals in the mid-Atlantic region had the highest RSRRs [0.98 percentage points higher than hospitals in the Mountain region; 95% confidence interval (CI), 0.84-1.12]. For-profit hospitals had an average RSRR 0.38 percentage points (95% CI, 0.24-0.53) higher than public hospitals. Both urban and rural hospitals had higher RSRRs than those in medium metropolitan areas. Hospitals without advanced cardiac surgery capability had an average RSRR 0.27 percentage points (95% CI, 0.18-0.36) higher than those with. The ratio of registered nurses per hospital bed was not associated with RSRR. Variability in RSRRs among hospitals of similar type was much larger than aggregate differences between types of hospitals.
Conclusions: Overall, larger, urban, academic facilities had modestly higher RSRRs than smaller, suburban, community hospitals, although there was a wide range of performance. The strong regional effect suggests that local practice patterns are an important influence. Disproportionately high readmission rates at for-profit hospitals may highlight the role of financial incentives favoring utilization.
Conflict of interest statement
Figures
References
-
- Donabedian A. The quality of care. How can it be assessed? JAMA. 1988;260(12):1743–1748. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
