

Acquired pendular nystagmus
- PMID: 28320194
- PMCID: PMC5363284
- DOI: 10.1016/j.jns.2017.01.033
Acquired pendular nystagmus
Abstract
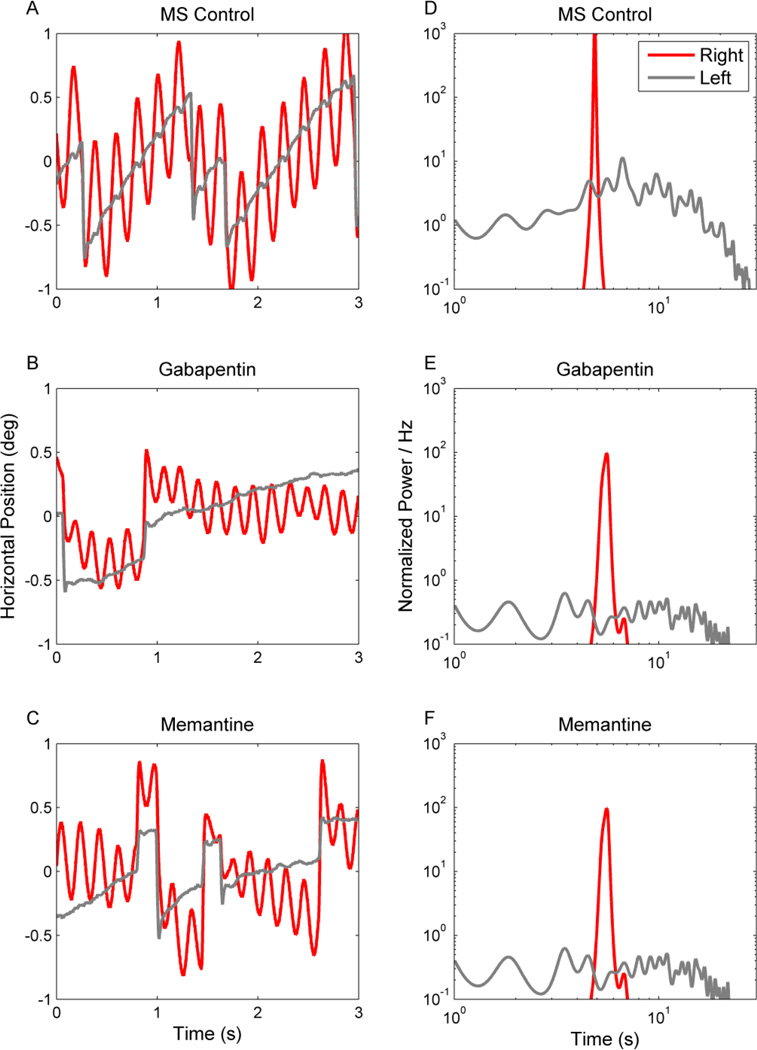
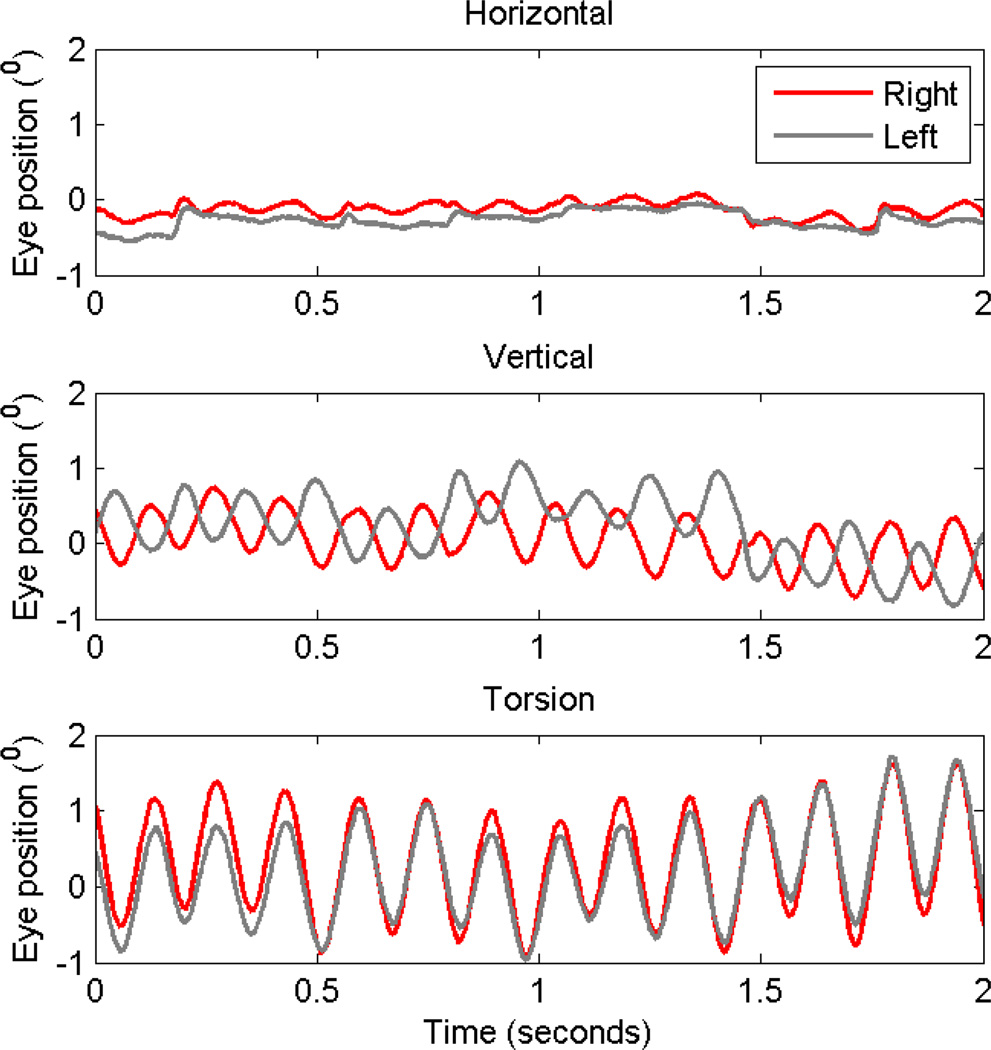
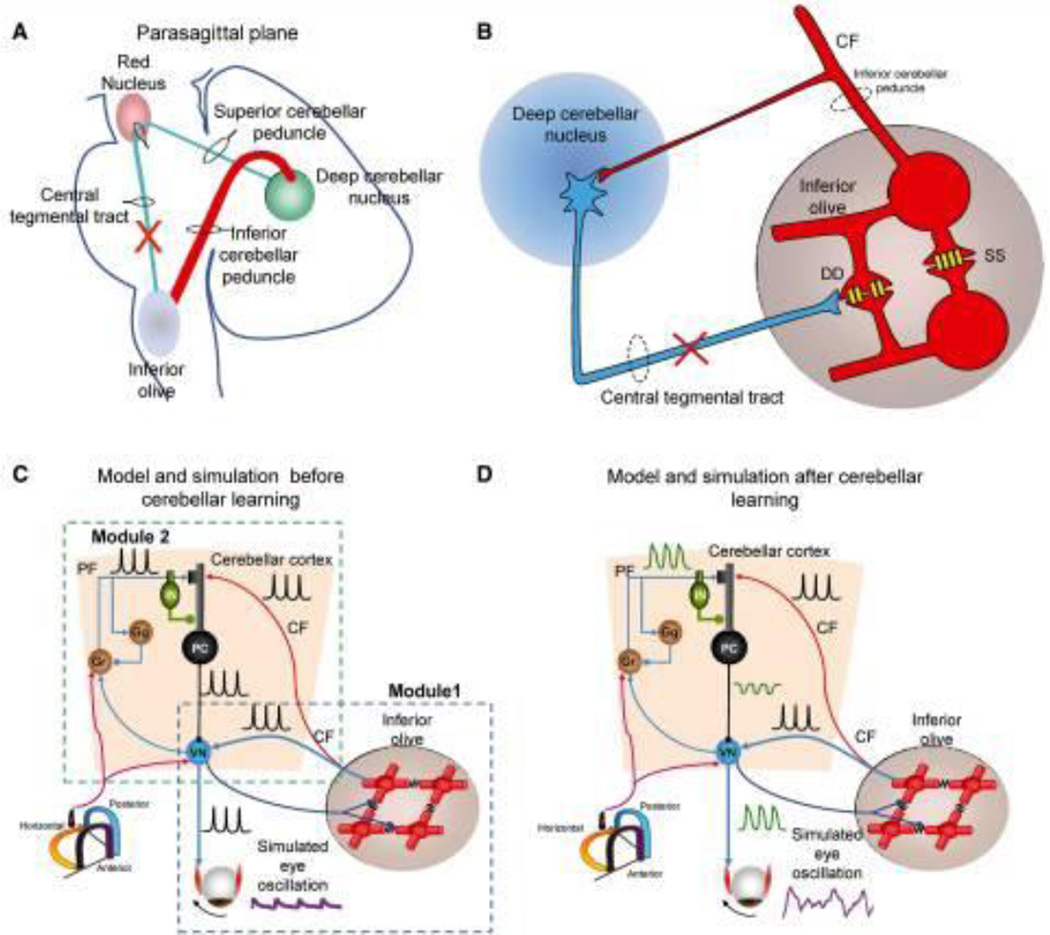
Acquired pendular nystagmus is comprised of quasi-sinusoidal oscillations of the eyes significantly affecting gaze holding and clarity of vision. The most common causes of acquired pendular nystagmus include demyelinating disorders such as multiple sclerosis and the syndrome of ocular palatal tremor. However, several other deficits, such as pharmacological intoxication, metabolic and genetic disorders, and granulomatous disorders can lead to syndromes mimicking acquired pendular nystagmus. Study of the kinematic features of acquired pendular nystagmus has suggested a putative pathophysiology of an otherwise mysterious neurological disorder. Here we review clinical features of neurological deficits that co-occur with acquired pendular nystagmus. Subsequent discussion of the pathophysiology of individual forms of pendular nystagmus speculates on mechanisms of the underlying disease while providing insights into pharmacotherapy of nystagmus.
Keywords: Degenerative disorder; Demyelination disorder; Multiple sclerosis; Stroke; Toxin exposure.
Copyright © 2017 Elsevier B.V. All rights reserved.
Figures
References
-
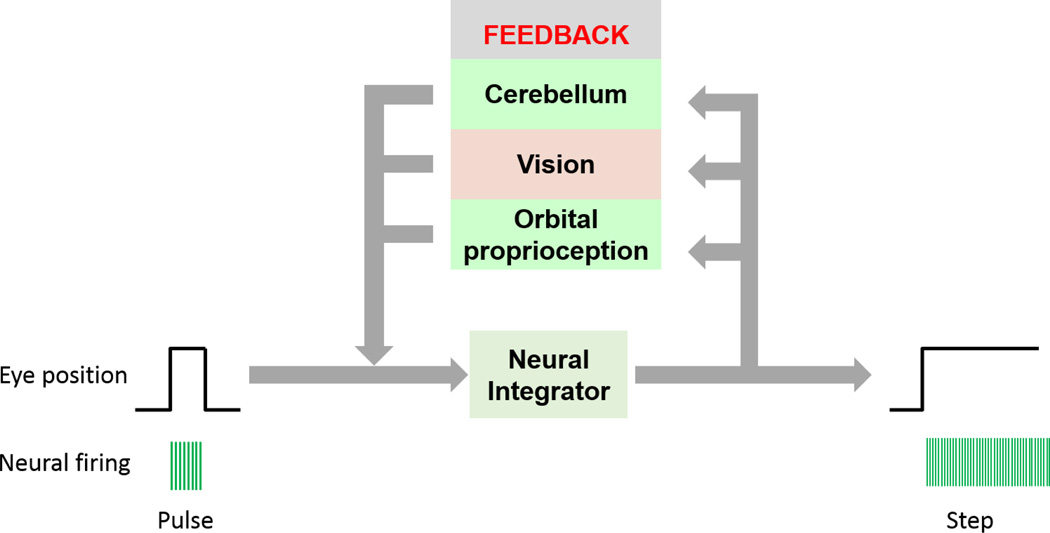
- Cannon SC, Robinson DA. An improved neural-network model for the neural integrator of the oculomotor system: more realistic neuron behavior. Biological cybernetics. 1985;53:93–108. - PubMed
-
- Cannon SC, Robinson DA. Loss of the neural integrator of the oculomotor system from brain stem lesions in monkey. Journal of neurophysiology. 1987;57:1383–1409. - PubMed
-
- Cannon SC, Robinson DA, Shamma S. A proposed neural network for the integrator of the oculomotor system. Biological cybernetics. 1983;49:127–136. - PubMed
-
- Robinson DA. The effect of cerebellectomy on the cat’s bestibulo-ocular integrator. Brain research. 1974;71:195–207. - PubMed
-
- Frohman EM, Frohman TC, Zee DS, McColl R, Galetta S. The neuro-ophthalmology of multiple sclerosis. The Lancet Neurology. 2005;4:111–121. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
