

Lipoprotein(a) and incident type-2 diabetes: results from the prospective Bruneck study and a meta-analysis of published literature
- PMID: 28320383
- PMCID: PMC5359972
- DOI: 10.1186/s12933-017-0520-z
Lipoprotein(a) and incident type-2 diabetes: results from the prospective Bruneck study and a meta-analysis of published literature
Abstract
Aims: We aimed to (1) assess the association between lipoprotein(a) [Lp(a)] concentration and incident type-2 diabetes in the Bruneck study, a prospective population-based study, and (2) combine findings with evidence from published studies in a literature-based meta-analysis.
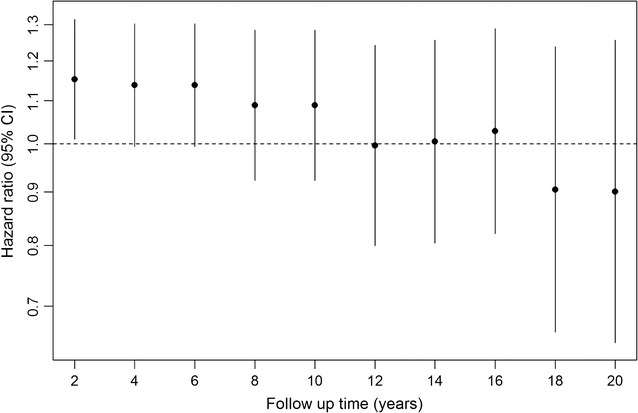
Methods: We used Cox proportional hazards models to calculate hazard ratios (HR) for incident type-2 diabetes over 20 years of follow-up in 815 participants of the Bruneck study according to their long-term average Lp(a) concentration. For the meta-analysis, we searched Medline, Embase and Web of Science for relevant prospective cohort studies published up to October 2016.
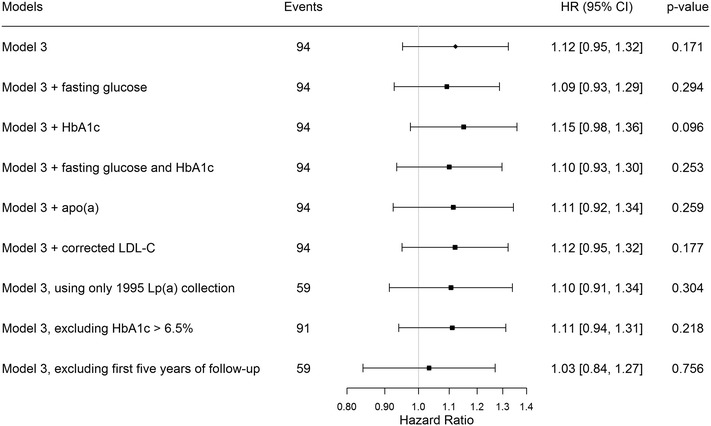
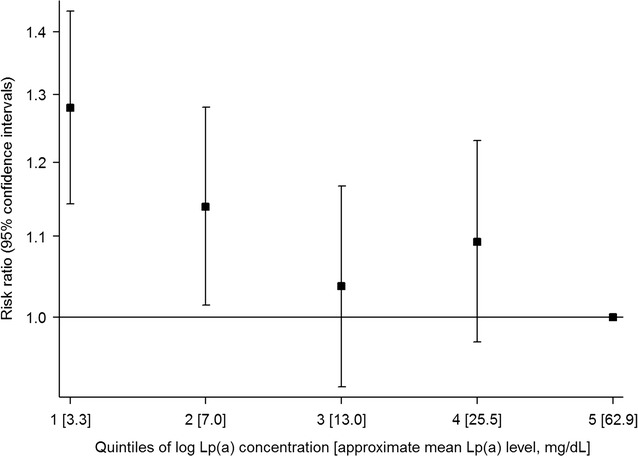
Results: In the Bruneck study, there was a 12% higher risk of type-2 diabetes for a one standard deviation lower concentration of log Lp(a) (HR = 1.12 [95% CI 0.95-1.32]; P = 0.171), after adjustment for age, sex, alcohol consumption, body mass index, smoking status, socioeconomic status, physical activity, systolic blood pressure, HDL cholesterol, log high-sensitivity C-reactive protein and waist-hip ratio. In a meta-analysis involving four prospective cohorts with a total of 74,575 participants and 4514 incident events, the risk of type-2 diabetes was higher in the lowest two quintiles of Lp(a) concentrations (weighted mean Lp(a) = 3.3 and 7.0 mg/dL, respectively) compared to the highest quintile (62.9 mg/dL), with the highest risk of type-2 diabetes seen in quintile 1 (HR = 1.28 [1.14-1.43]; P < 0.001).
Conclusions: The current available evidence from prospective studies suggests that there is an inverse association between Lp(a) concentration and risk of type-2 diabetes, with a higher risk of type-2 diabetes at low Lp(a) concentrations (approximately <7 mg/dL).
Keywords: Diabetes; Lipoprotein(a); Meta-analysis; Prospective study.
Figures
References
-
- Seed M, Hoppichler F, Reaveley D, McCarthy S, Thompson GR, Boerwinkle E, Utermann G. Relation of serum lipoprotein(a) concentration and apolipoprotein(a) phenotype to coronary heart disease in patients with familial hypercholesterolemia. N Engl J Med. 1990;322(21):1494–1499. doi: 10.1056/NEJM199005243222104. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
