

Effect of Uric Acid Lowering on Renin-Angiotensin-System Activation and Ambulatory BP: A Randomized Controlled Trial
- PMID: 28320765
- PMCID: PMC5477221
- DOI: 10.2215/CJN.10771016
Effect of Uric Acid Lowering on Renin-Angiotensin-System Activation and Ambulatory BP: A Randomized Controlled Trial
Abstract
Background and objectives: Higher serum uric acid levels, even within the reference range, are strongly associated with increased activity of the renin-angiotensin system (RAS) and risk of incident hypertension. However, the effect of lowering serum uric acid on RAS activity in humans is unknown, although the data that lowering serum uric acid can reduce BP are conflicting.
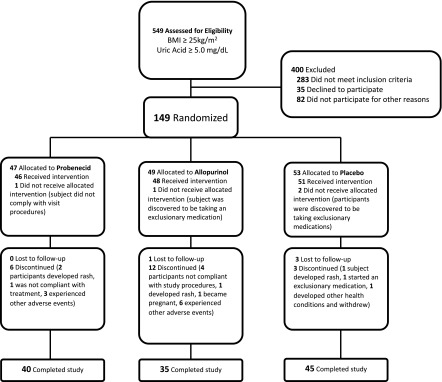
Design, setting, participants, & measurements: In a double-blind placebo-controlled trial conducted from 2011 to 2015, we randomly assigned 149 overweight or obese adults with serum uric acid ≥5.0 mg/dl to uric acid lowering with either probenecid or allopurinol, or to placebo. The primary endpoints were kidney-specific and systemic RAS activity. Secondary endpoints included mean 24-hour systolic BP, mean awake and asleep BP, and nocturnal dipping.
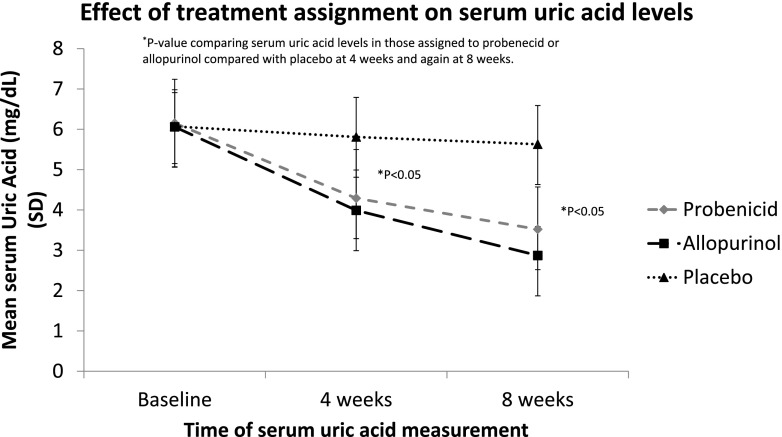
Results: Allopurinol and probenecid markedly lowered serum uric acid after 4 and 8 weeks compared with placebo (mean serum uric acid in allopurinol, probenecid, and placebo at 8 weeks was 2.9, 3.5, and 5.6 mg/dl, respectively). The change in kidney-specific RAS activity, measured as change in the median (interquartile range) renal plasma flow response to captopril (in ml/min per 1.73 m2) from baseline to 8 weeks, was -4 (-25 to 32) in the probenecid group (P=0.83), -4 (-16 to 9) in the allopurinol group (P=0.32), and 1 (-21 to 17) in the placebo group (P=0.96), with no significant treatment effect (P=0.77). Similarly, plasma renin activity and plasma angiotensin II levels did not significantly change with treatment. The change in mean (±SD) 24-hour systolic BPs from baseline to 8 weeks was -1.6±10.1 with probenecid (P=0.43), -0.4±6.1 with allopurinol (P=0.76), and 0.5±6.0 with placebo (P=0.65); there was no significant treatment effect (P=0.58). Adverse events occurred in 9%, 12%, and 2% of those given probenecid, allopurinol, or placebo, respectively.
Conclusions: In contrast to animal experiments and observational studies, this randomized, placebo-controlled trial found that uric acid lowering had no effect on kidney-specific or systemic RAS activity after 8 weeks or on mean systolic BP. These data do not support the hypothesis that higher levels of uric acid are a reversible risk factor for increased BP.
Keywords: BP; Uric acid; allopurinol; placebo controlled; probenecid; randomized controlled trials; renin angiotensin system; urate; urate lowering therapy.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Abiko H, Konta T, Hao Z, Takasaki S, Suzuki K, Ichikawa K, Ikeda A, Shibata Y, Takeishi Y, Kawata S, Kato T, Kubota I: Factors correlated with plasma renin activity in general Japanese population. Clin Exp Nephrol 13: 130–137, 2009 - PubMed
-
- Perlstein TS, Gumieniak O, Hopkins PN, Murphey LJ, Brown NJ, Williams GH, Hollenberg NK, Fisher ND: Uric acid and the state of the intrarenal renin-angiotensin system in humans. Kidney Int 66: 1465–1470, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
