

Effectiveness of chronic care models for the management of type 2 diabetes mellitus in Europe: a systematic review and meta-analysis
- PMID: 28320788
- PMCID: PMC5372084
- DOI: 10.1136/bmjopen-2016-013076
Effectiveness of chronic care models for the management of type 2 diabetes mellitus in Europe: a systematic review and meta-analysis
Abstract
Objectives: We evaluated the effectiveness of European chronic care programmes for type 2 diabetes mellitus (characterised by integrative care and a multicomponent framework for enhancing healthcare delivery), compared with usual diabetes care.
Design: Systematic review and meta-analysis.
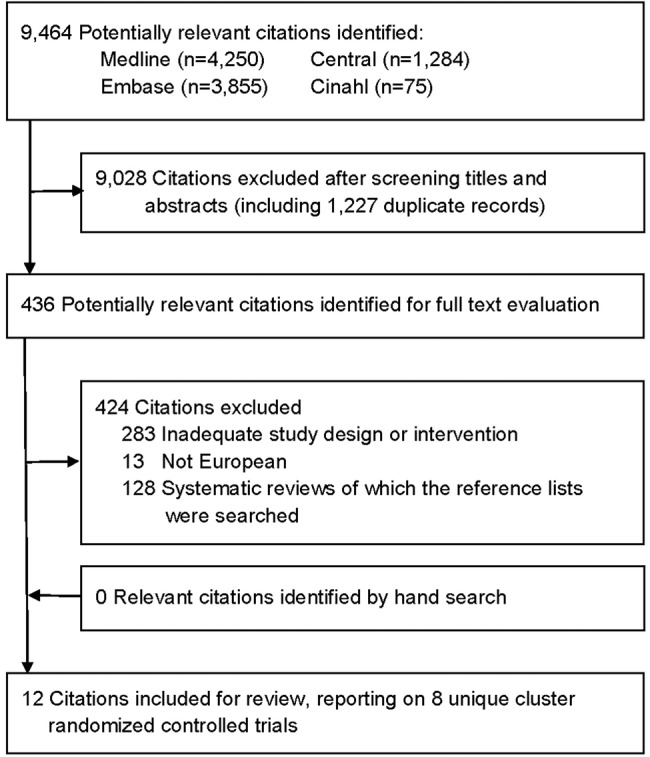
Data sources: MEDLINE, Embase, CENTRAL and CINAHL from January 2000 to July 2015.
Eligibility criteria: Randomised controlled trials focussing on (1) adults with type 2 diabetes, (2) multifaceted diabetes care interventions specifically designed for type 2 diabetes and delivered in primary or secondary care, targeting patient, physician and healthcare organisation and (3) usual diabetes care as the control intervention.
Data extraction: Study characteristics, characteristics of the intervention, data on baseline demographics and changes in patient outcomes.
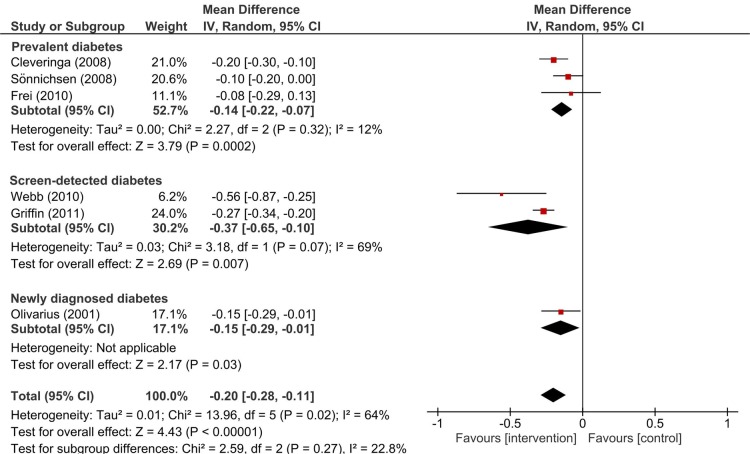
Data analysis: Weighted mean differences in change in HbA1c and total cholesterol levels between intervention and control patients (95% CI) were estimated using a random-effects model.
Results: Eight cluster randomised controlled trials were identified for inclusion (9529 patients). One year of multifaceted care improved HbA1c levels in patients with screen-detected and newly diagnosed diabetes, but not in patients with prevalent diabetes, compared to usual diabetes care. Across all seven included trials, the weighted mean difference in HbA1c change was -0.07% (95% CI -0.10 to -0.04) (-0.8 mmol/mol (95% CI -1.1 to -0.4)); I2=21%. The findings for total cholesterol, LDL-cholesterol and blood pressure were similar to HbA1c, albeit statistical heterogeneity between studies was considerably larger. Compared to usual care, multifaceted care did not significantly change quality of life of the diabetes patient. Finally, measured for screen-detected diabetes only, the risk of macrovascular and mircovascular complications at follow-up was not significantly different between intervention and control patients.
Conclusions: Effects of European multifaceted diabetes care patient outcomes are only small. Improvements are somewhat larger for screen-detected and newly diagnosed diabetes patients than for patients with prevalent diabetes.
Keywords: Europe; Managed care; Meta-analysis; Systematic review; Type 2 diabetes mellitus.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Figures

References
-
- Wagner EH, Davis C, Schaefer J et al. . A survey of leading chronic disease management programs: are they consistent with the literature? Manag Care Q 1999;7:56–66. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical