

Exploratory analysis of osteoarthritis progression among medication users: data from the Osteoarthritis Initiative
- PMID: 28321269
- PMCID: PMC5322858
- DOI: 10.1177/1759720X16664323
Exploratory analysis of osteoarthritis progression among medication users: data from the Osteoarthritis Initiative
Abstract
Background: We conducted an exploratory analysis of osteoarthritis progression among medication users in the Osteoarthritis Initiative to identify interventions or pathways that may be associated with disease modification and therefore of interest for future clinical trials.
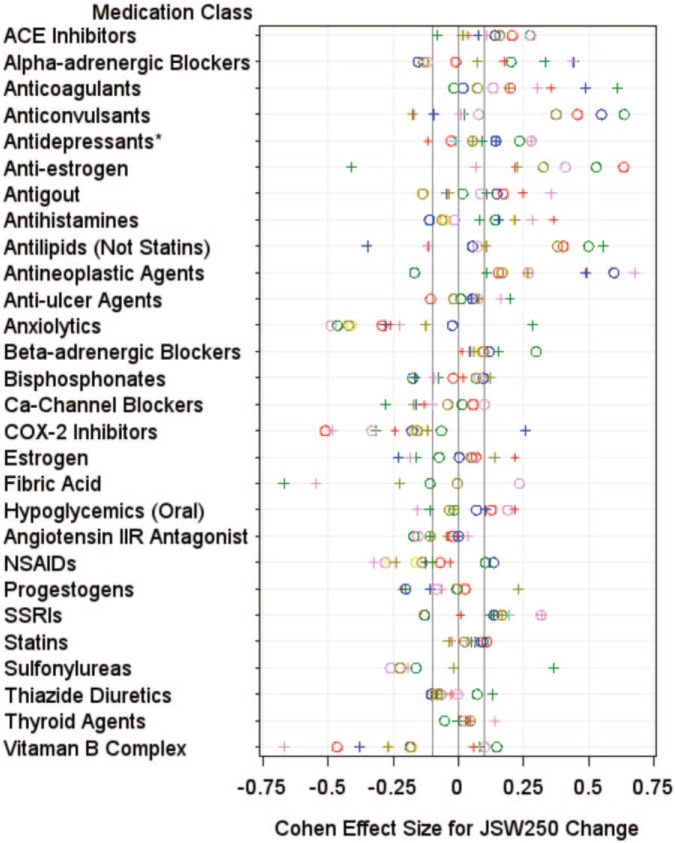
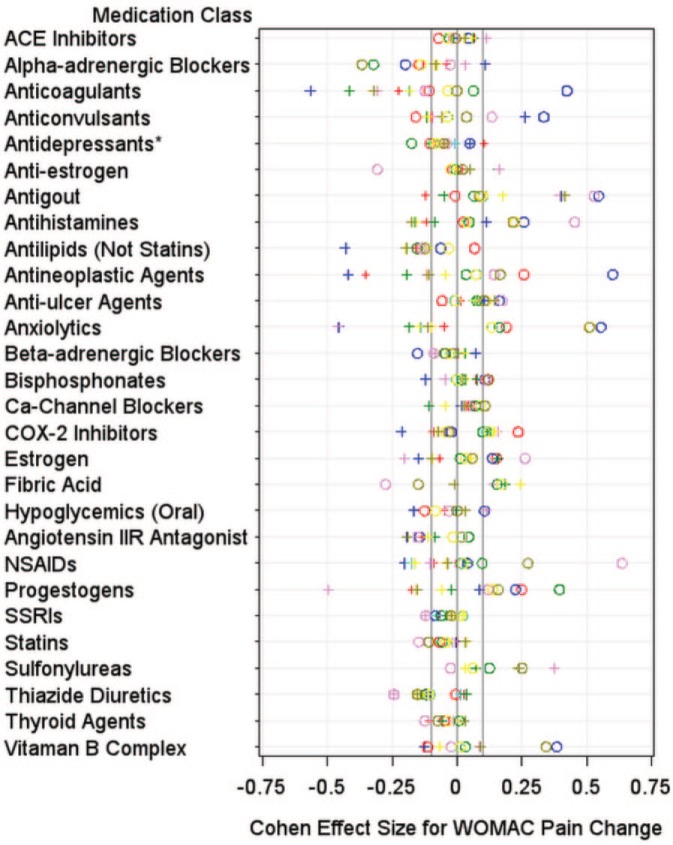
Methods: We used participants from the Osteoarthritis Initiative with annual medication inventory data between the baseline and 36-month follow-up visit (n = 2938). Consistent medication users were defined for each medication classification as a participant reporting at all four annual visits that they were regularly using an oral prescription medication at the time of the visit. The exploratory analysis focused on medication classes with 40 or more users. The primary outcome measures were medial tibiofemoral joint space width change and the Western Ontario and McMaster Universities Arthritis Index (WOMAC) knee pain score change (12-36-month visits). Within each knee, we explored eight comparisons between users and matched or unmatched nonusers (defined two ways). An effect size of each comparison was calculated. Medication classes had potential signals if (a) both knees had less progression among users compared with nonusers, or (b) there was less progression based on structure and symptoms in one knee.
Results: We screened 28 medication classes. Six medication classes had signals for fewer structural changes and better knee pain changes: alpha-adrenergic blockers, antilipemic (excluding statins and fibric acid), anticoagulants, selective serotonin reuptake inhibitors, antihistamines, and antineoplastic agents. Four medication classes had signals for structural changes alone: anti-estrogen (median effect size = 0.28; range = -0.41-0.64), angiotensin-converting enzyme inhibitors (median effect size = 0.13; range = -0.08-0.28), beta-adrenergic blockers (median effect size = 0.09; range = 0.01-0.30), and thyroid agents (median effect size = 0.04; range = -0.05-0.14). Thiazide diuretics had evidence for symptom modification (median effect size = -0.12; range = -0.24-0.04).
Conclusions: Users of neurovascular, antilipemic, or hormonal interventions may have less disease progression compared with nonusers.
Keywords: knee; pain; radiographs.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Abourazzak F., Talbi S., Lazrak F., Azzouzi H., Aradoini N., Keita S., Errasfa M., Harzy T. (2015) Does metabolic syndrome or its individual components affect pain and function in knee osteoarthritis women? Curr Rheumatol Rev 11: 8–14. PMID: 26002459. - PubMed
-
- Bergman A., Willen H., Lindstrand A., Pettersson H. (1994) Osteoarthritis of the knee: correlation of subchondral MR signal abnormalities with histopathologic and radiographic features. Skeletal Radiol 23: 445–448. - PubMed
-
- Borovikova L., Ivanova S., Zhang M., Yang H., Botchkina G., Watkins L., et al. (2000) Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature 405: 458–462. - PubMed
-
- Clockaerts S., Van Osch G., Bastiaansen-Jenniskens Y., Verhaar J., Van Glabbeek F., Van Meurs J., et al. (2011) Statin use is associated with reduced incidence and progression of knee osteoarthritis in the Rotterdam study. Ann Rheum Dis 71: 642–647. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
