

Prognosis of cirrhotic patients admitted to intensive care unit: a meta-analysis
- PMID: 28321803
- PMCID: PMC5359266
- DOI: 10.1186/s13613-017-0249-6
Prognosis of cirrhotic patients admitted to intensive care unit: a meta-analysis
Abstract
Background: The best predictors of short- and medium-term mortality of cirrhotic patients receiving intensive care support are unknown.
Methods: We conducted meta-analyses from 13 studies (2523 cirrhotics) after selection of original articles and response to a standardized questionnaire by the corresponding authors. End-points were in-ICU, in-hospital, and 6-month mortality in ICU survivors. A total of 301 pooled analyses, including 95 analyses restricted to 6-month mortality among ICU survivors, were conducted considering 249 variables (including reason for admission, organ replacement therapy, and composite prognostic scores).
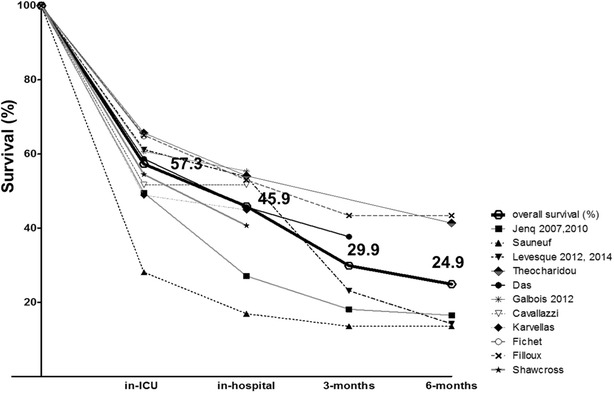
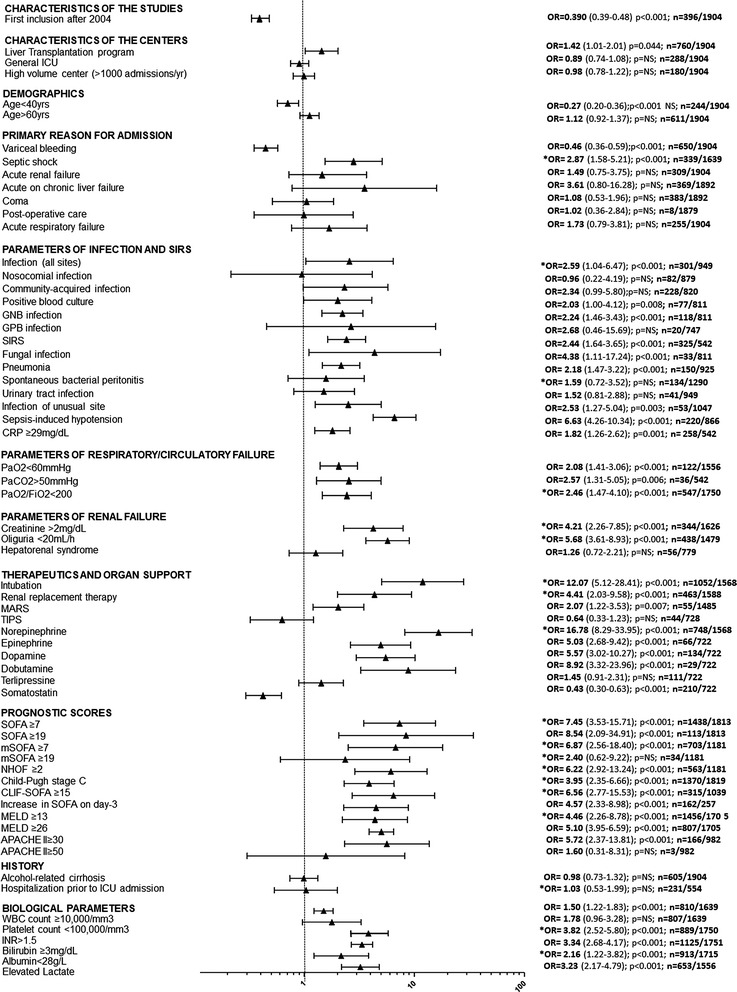
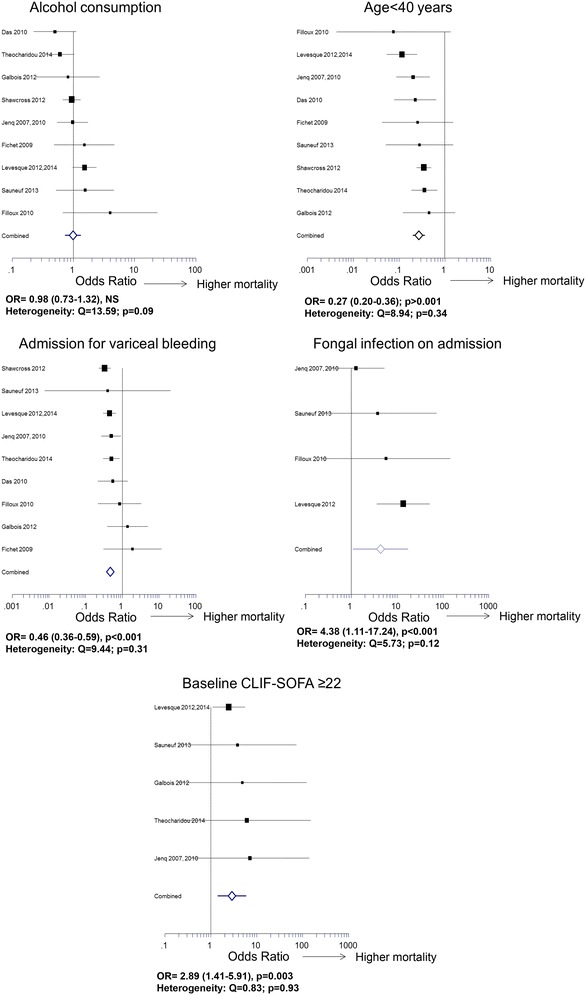
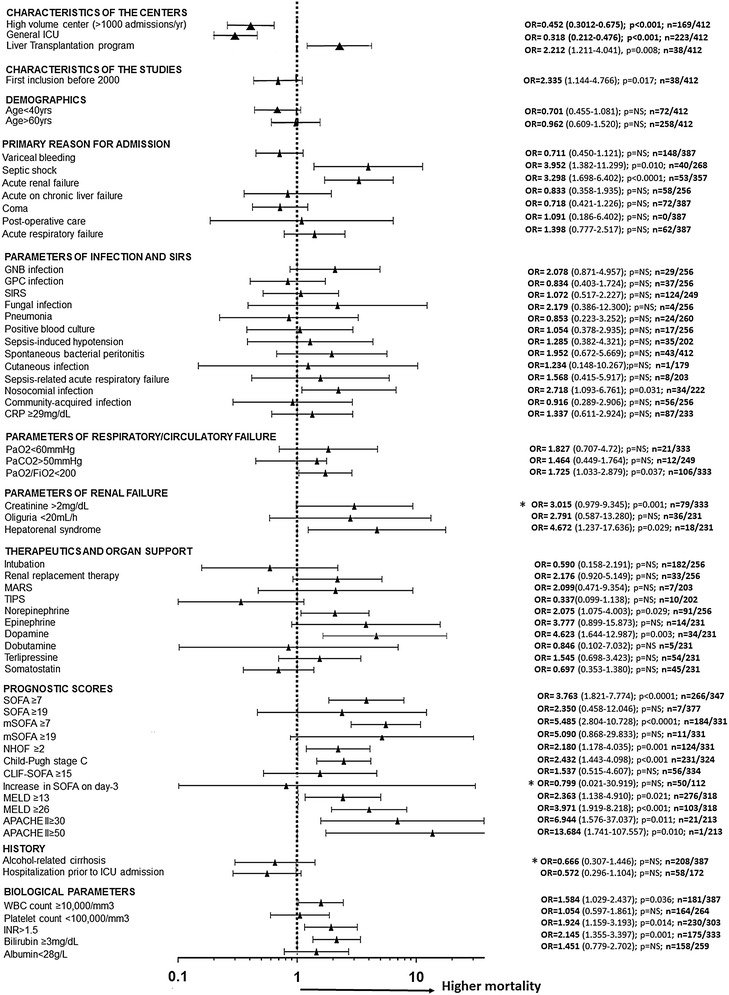
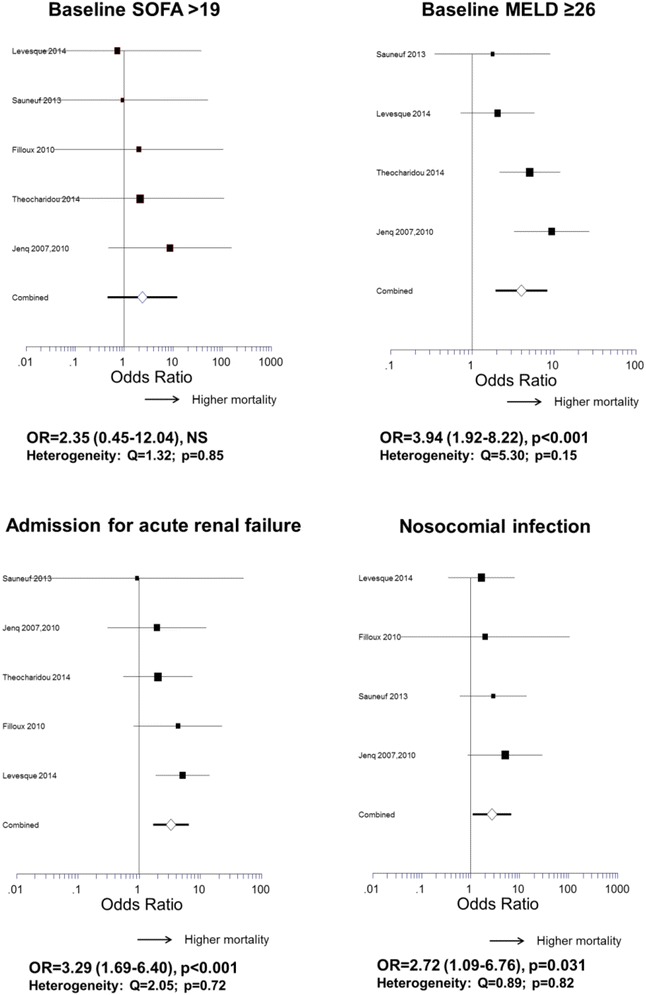
Results: In-ICU, in-hospital, and 6-month mortality was 42.7, 54.1, and 75.1%, respectively. Forty-eight patients (3.8%) underwent liver transplantation during follow-up. In-ICU mortality was lower in patients admitted for variceal bleeding (OR 0.46; 95% CI 0.36-0.59; p < 0.001) and higher in patients with SOFA > 19 at baseline (OR 8.54; 95% CI 2.09-34.91; p < 0.001; PPV = 0.93). High SOFA no longer predicted mortality at 6 months in ICU survivors. Twelve variables related to infection were predictors of in-ICU mortality, including SIRS (OR 2.44; 95% CI 1.64-3.65; p < 0.001; PPV = 0.57), pneumonia (OR 2.18; 95% CI 1.47-3.22; p < 0.001; PPV = 0.69), sepsis-associated refractory oliguria (OR 10.61; 95% CI 4.07-27.63; p < 0.001; PPV = 0.76), and fungal infection (OR 4.38; 95% CI 1.11-17.24; p < 0.001; PPV = 0.85). Among therapeutics, only dopamine (OR 5.57; 95% CI 3.02-10.27; p < 0.001; PPV = 0.68), dobutamine (OR 8.92; 95% CI 3.32-23.96; p < 0.001; PPV = 0.86), epinephrine (OR 5.03; 95% CI 2.68-9.42; p < 0.001; PPV = 0.77), and MARS (OR 2.07; 95% CI 1.22-3.53; p = 0.007; PPV = 0.58) were associated with in-ICU mortality without heterogeneity. In ICU survivors, eight markers of liver and renal failure predicted 6-month mortality, including Child-Pugh stage C (OR 2.43; 95% CI 1.44-4.10; p < 0.001; PPV = 0.57), baseline MELD > 26 (OR 3.97; 95% CI 1.92-8.22; p < 0.0001; PPV = 0.75), and hepatorenal syndrome (OR 4.67; 95% CI 1.24-17.64; p = 0.022; PPV = 0.88).
Conclusions: Prognosis of cirrhotic patients admitted to ICU is poor since only a minority undergo liver transplant. The prognostic performance of general ICU scores decreases over time, unlike the Child-Pugh and MELD scores, even recorded in the context of organ failure. Infection-related parameters had a short-term impact, whereas liver and renal failure had a sustained impact on mortality.
Keywords: CLIF-SOFA; Cirrhosis; Extrahepatic organ failure; MELD; Mortality; Organ replacement therapy; Prognostic scores.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
