

Impact of Insurance Provider on Overall Costs in Failed Back Surgery Syndrome: A Cost Study of 122,827 Patients
- PMID: 28322477
- PMCID: PMC5482408
- DOI: 10.1111/ner.12584
Impact of Insurance Provider on Overall Costs in Failed Back Surgery Syndrome: A Cost Study of 122,827 Patients
Abstract
Objectives: Failed back surgery syndrome (FBSS) affects 40% of patients following spine surgery with estimated costs of $20 billion to the US health care system. The aim of this study was to assess the cost differences across the different insurance providers for FBSS patients.
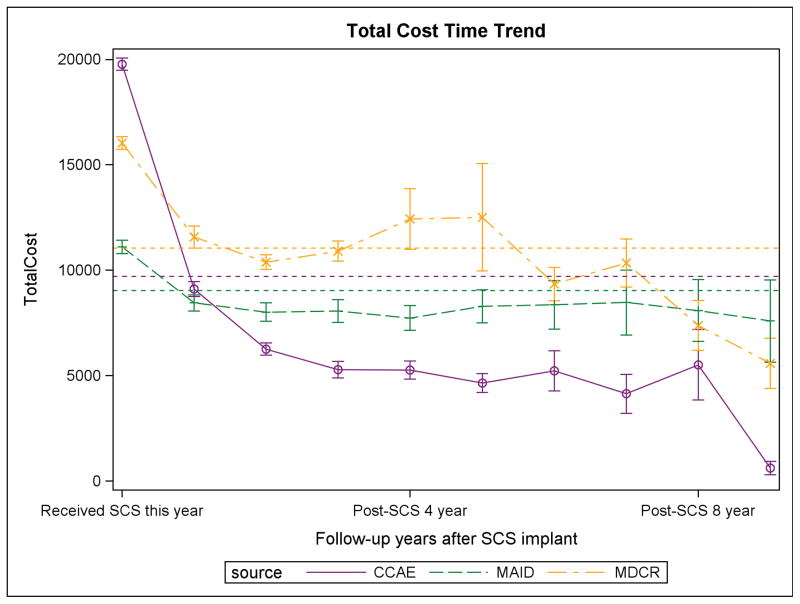
Methods: A retrospective longitudinal study was performed using the Truven MarketScan® database to identify FBSS patients from 2001 to 2012. Patients were grouped into Commercial, Medicaid, or Medicare cohorts. We collected one-year prior to FBSS diagnosis (baseline), then at year of spinal cord stimulation (SCS)-implantation and nine-year post-SCS implantation cost outcomes.
Results: We identified 122,827 FBSS patients, with 117,499 patients who did not undergo an SCS-implantation (Commercial: n = 49,075, Medicaid: n = 23,180, Medicare: n = 45,244) and 5328 who did undergo an SCS implantation (Commercial: n = 2279, Medicaid: n = 1003, Medicare: n = 2046). Baseline characteristics were similar between the cohorts, with the Medicare-cohort being significantly older. Over the study period, there were significant differences in overall cost metrics between the cohorts who did not undergo SCS implantation with the Medicaid-cohort had the lowest annual median (interquartile range) total cost (Medicaid: $4530.4 [$1440.6, $11,973.5], Medicare: $7292.0 [$3371.4, $13,989.4], Commercial: $4944.3 [$363.8, $13,294.0], p < 0.0001). However, when comparing the patients who underwent SCS implantation, the commercial-cohort had the lowest annual median (interquartile range) total costs (Medicaid: $4045.6 [$1146.9, $11,533.9], Medicare: $7158.1 [$3160.4, $13,916.6], Commercial: $2098.1 [$0.0, $8919.6], p < 0.0001).
Conclusions: Our study demonstrates a significant difference in overall costs between various insurance providers in the management of FBSS, with Medicaid-insured patients having lower overall costs compared to Commercial- and Medicare-patients. SCS is cost-effective across all insurance groups (Commercial > Medicaid > Medicare) beginning at two years and continuing through nine-year follow-up. Further studies are necessary to understand the cost differences between these insurance providers, in hopes of reducing unnecessary health care expenditures for patients with FBSS.
Keywords: Cost; FBSS; Medicaid; Medicare; SCS; insurance disparities.
© 2017 International Neuromodulation Society.
Conflict of interest statement
Conflict of Interest Statement: Shivanand Lad, MD, PhD, has received fees for serving as a speaker and consultant for Medtronic Inc., Boston Scientific, and St. Jude Medical. He serves as the Director of the Duke Neuro-outcomes Center, which has received research funding from NIH KM1 CA 156687, Medtronic Inc. and St. Jude Medical. The remaining authors report no conflicts of interest or financial disclosures.
Figures
References
-
- Schmidt CO, Raspe H, Pfingsten M, et al. Back pain in the German adult population: prevalence, severity, and sociodemographic correlates in a multiregional survey. Spine. 2007;32(18):2005–2011. - PubMed
-
- Patel AT, Ogle AA. Diagnosis and management of acute low back pain. American family physician. 2000;61(6):1779–1786. 1789–1790. - PubMed
-
- Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. The spine journal: official journal of the North American Spine Society. 2008;8(1):8–20. - PubMed
-
- Chan CW, Peng P. Failed back surgery syndrome. Pain medicine. 2011;12(4):577–606. - PubMed
-
- Taylor RS, Ryan J, O’Donnell R, Eldabe S, Kumar K, North RB. The cost-effectiveness of spinal cord stimulation in the treatment of failed back surgery syndrome. The Clinical journal of pain. 2010;26(6):463–469. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
