

Constipation-Predominant Irritable Bowel Syndrome Females Have Normal Colonic Barrier and Secretory Function
- PMID: 28323272
- PMCID: PMC5502210
- DOI: 10.1038/ajg.2017.48
Constipation-Predominant Irritable Bowel Syndrome Females Have Normal Colonic Barrier and Secretory Function
Abstract
Objectives: The objective of this study was to determine whether constipation-predominant irritable bowel syndrome (IBS-C) is associated with changes in intestinal barrier and secretory function.
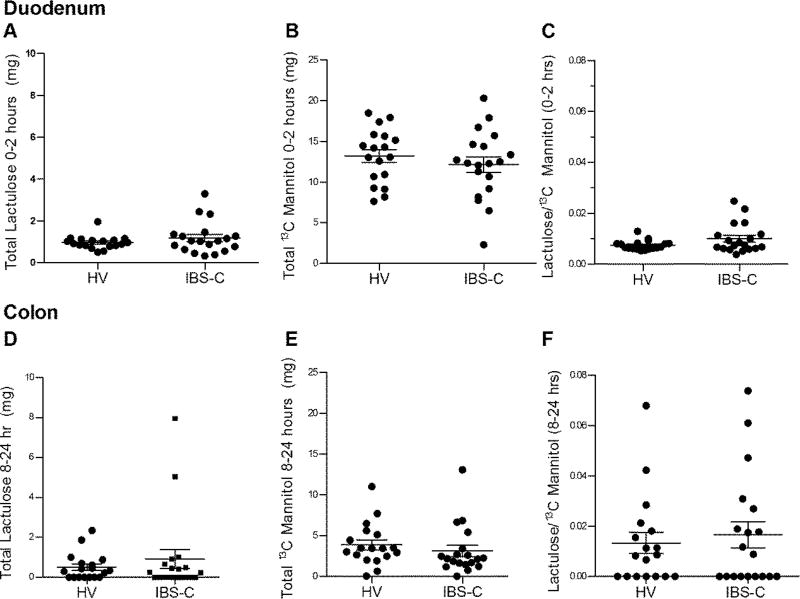
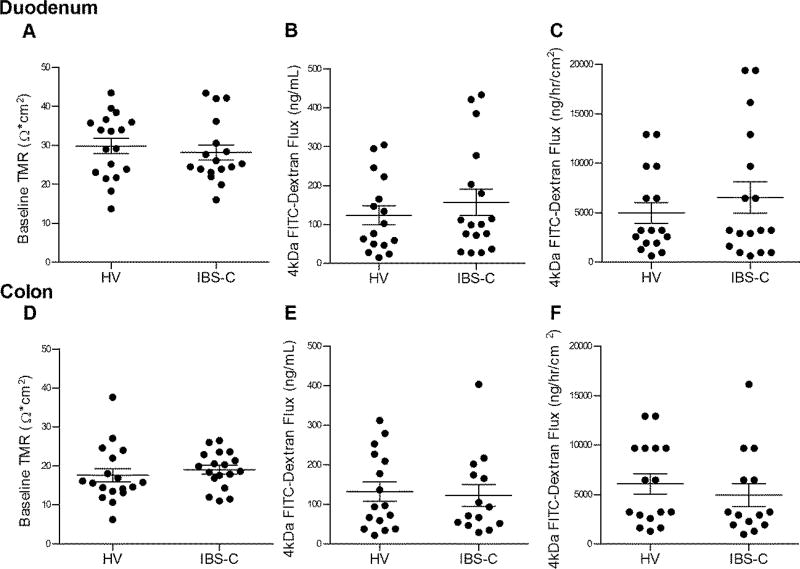
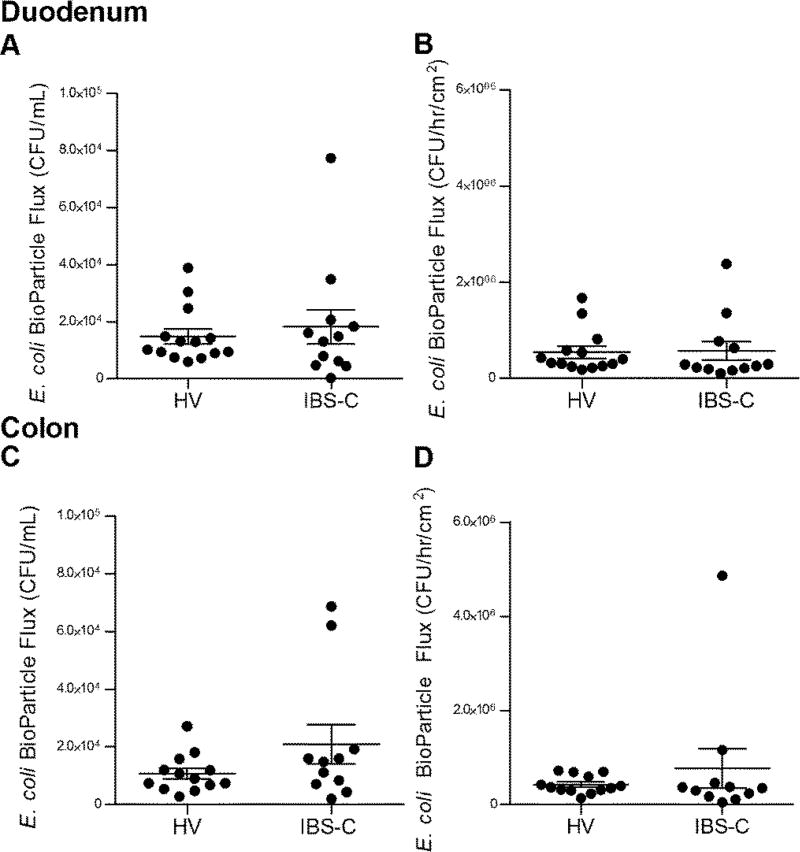
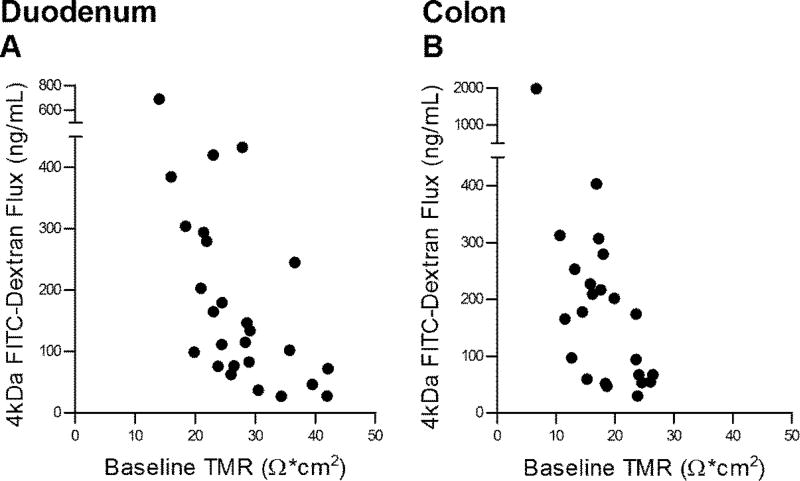
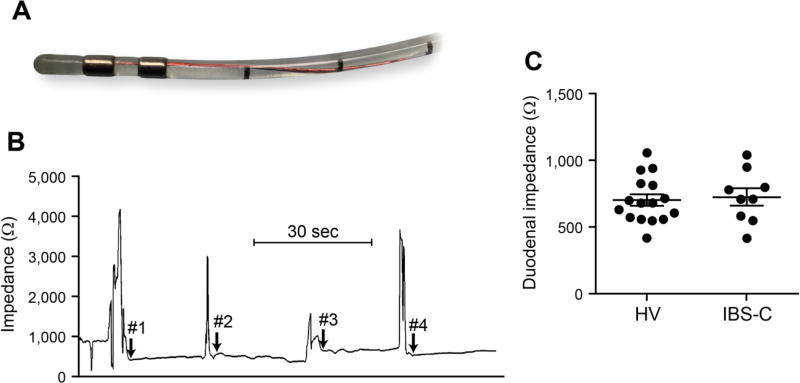
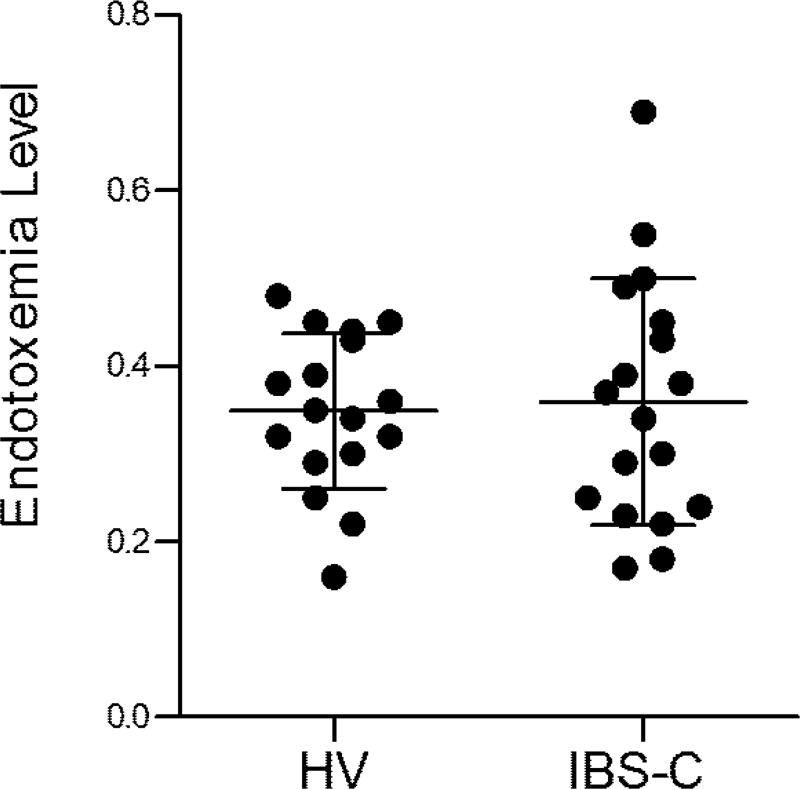
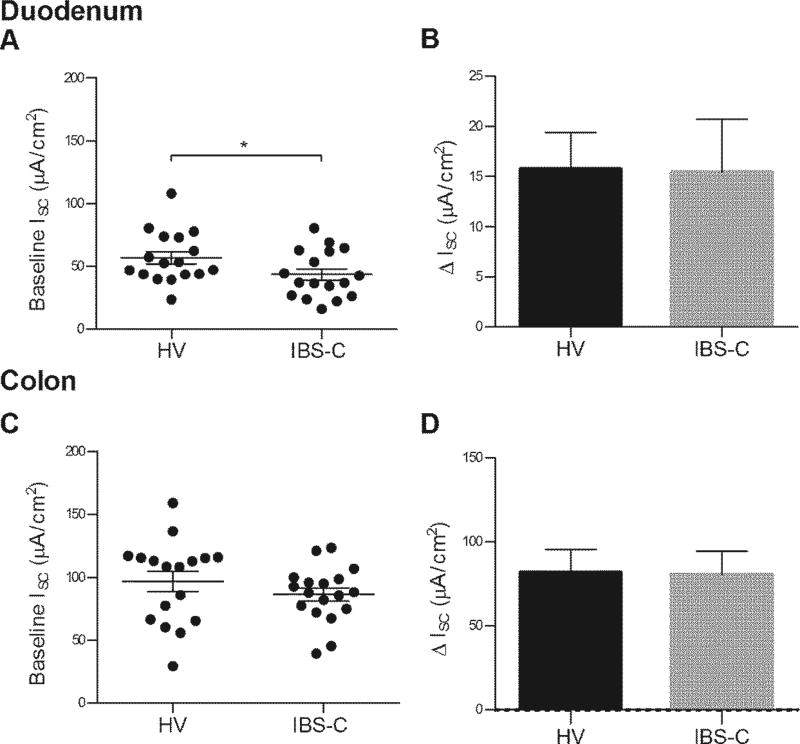
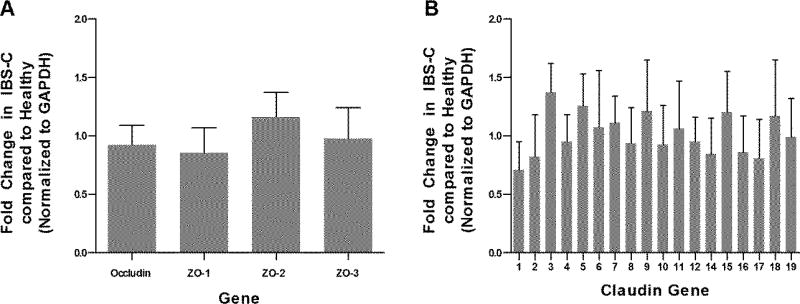
Methods: A total of 19 IBS-C patients and 18 healthy volunteers (all females) underwent saccharide excretion assay (0.1 g 13C mannitol and 1 g lactulose), measurements of duodenal and colonic mucosal barrier (transmucosal resistance (TMR), macromolecular and Escherichia coli Bio-Particle translocation), mucosal secretion (basal and acetylcholine (Ach)-evoked short-circuit current (Isc)), in vivo duodenal mucosal impedance, circulating endotoxins, and colonic tight junction gene expression.
Results: There were no differences in the in vivo measurements of barrier function between IBS-C patients and healthy controls: cumulative excretion of 13C mannitol (0-2 h mean (s.e.m.); IBS-C: 12.1 (0.9) mg vs. healthy: 13.2 (0.8) mg) and lactulose (8-24 h; IBS-C: 0.9 (0.5) mg vs. healthy: 0.5 (0.2) mg); duodenal impedance IBS-C: 729 (65) Ω vs. healthy: 706 (43) Ω; plasma mean endotoxin activity level IBS-C: 0.36 (0.03) vs. healthy: 0.35 (0.02); and in colonic mRNA expression of occludin, zonula occludens (ZO) 1-3, and claudins 1-12 and 14-19. The ex vivo findings were consistent, with no group differences: duodenal TMR (IBS-C: 28.2 (1.9) Ω cm2 vs. healthy: 29.8 (1.9) Ω cm2) and colonic TMR (IBS-C: 19.1 (1.1) Ω cm2 vs. healthy: 17.6 (1.7) Ω cm2); fluorescein isothiocyanate (FITC)-dextran (4 kDa) and E. coli Bio-Particle flux. Colonic basal Isc was similar, but duodenal basal Isc was lower in IBS-C (43.5 (4.5) μA cm-2) vs. healthy (56.9 (4.9) μA cm-2), P=0.05. Ach-evoked ΔIsc was similar.
Conclusions: Females with IBS-C have normal colonic barrier and secretory function. Basal duodenal secretion is decreased in IBS-C.
Conflict of interest statement
Figures
References
-
- Piche T. Tight junctions and IBS--the link between epithelial permeability, low-grade inflammation, and symptom generation? Neurogastroenterol Motil. 2014;26:296–302. - PubMed
-
- Piche T, Barbara G, Aubert P, et al. Impaired intestinal barrier integrity in the colon of patients with irritable bowel syndrome: involvement of soluble mediators. Gut. 2009;58:196–201. - PubMed
-
- Vivinus-Nebot M, Dainese R, Anty R, et al. Combination of allergic factors can worsen diarrheic irritable bowel syndrome: role of barrier defects and mast cells. Am J Gastroenterol. 2012;107:75–81. - PubMed
-
- Annahazi A, Ferrier L, Bezirard V, et al. Luminal cysteine-proteases degrade colonic tight junction structure and are responsible for abdominal pain in constipation-predominant IBS. Am J Gastroenterol. 2013;108:1322–31. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
