

Incretin Therapies Do Not Expand β-Cell Mass or Alter Pancreatic Histology in Young Male Mice
- PMID: 28323942
- PMCID: PMC5460937
- DOI: 10.1210/en.2017-00027
Incretin Therapies Do Not Expand β-Cell Mass or Alter Pancreatic Histology in Young Male Mice
Abstract
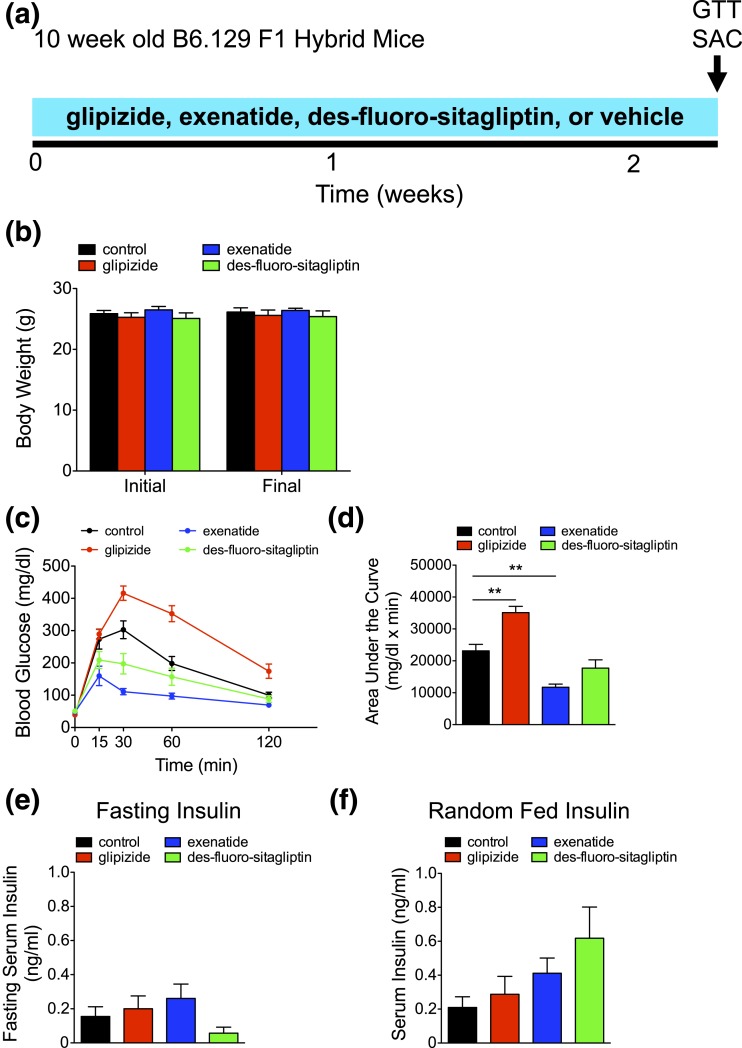
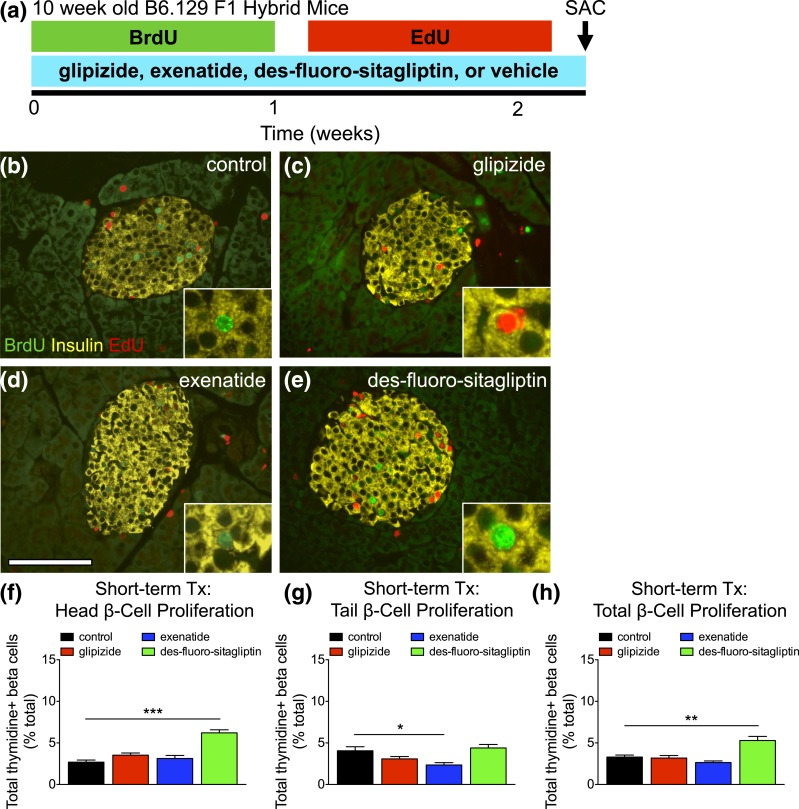
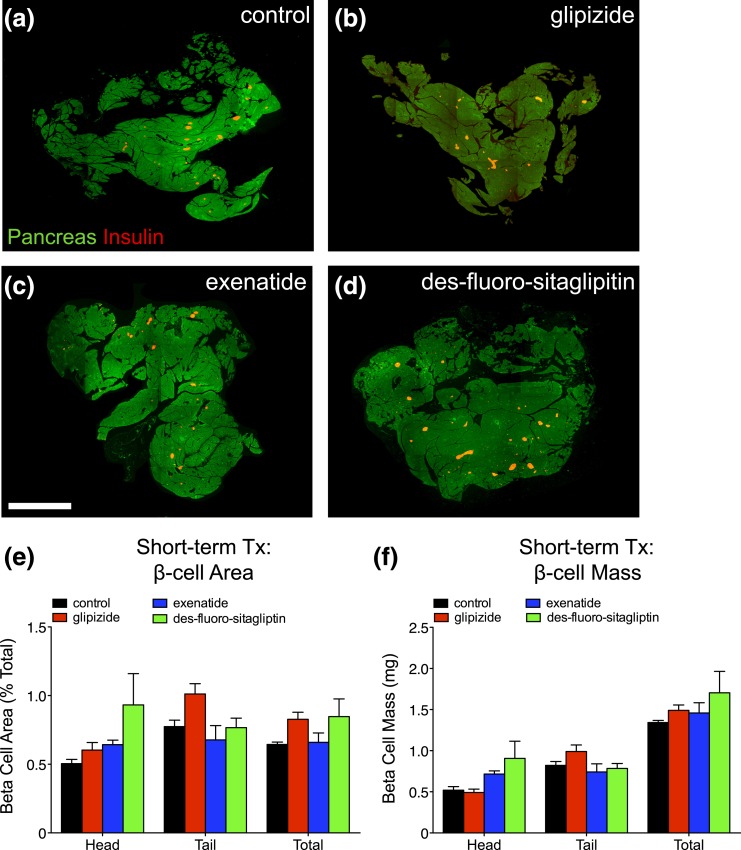
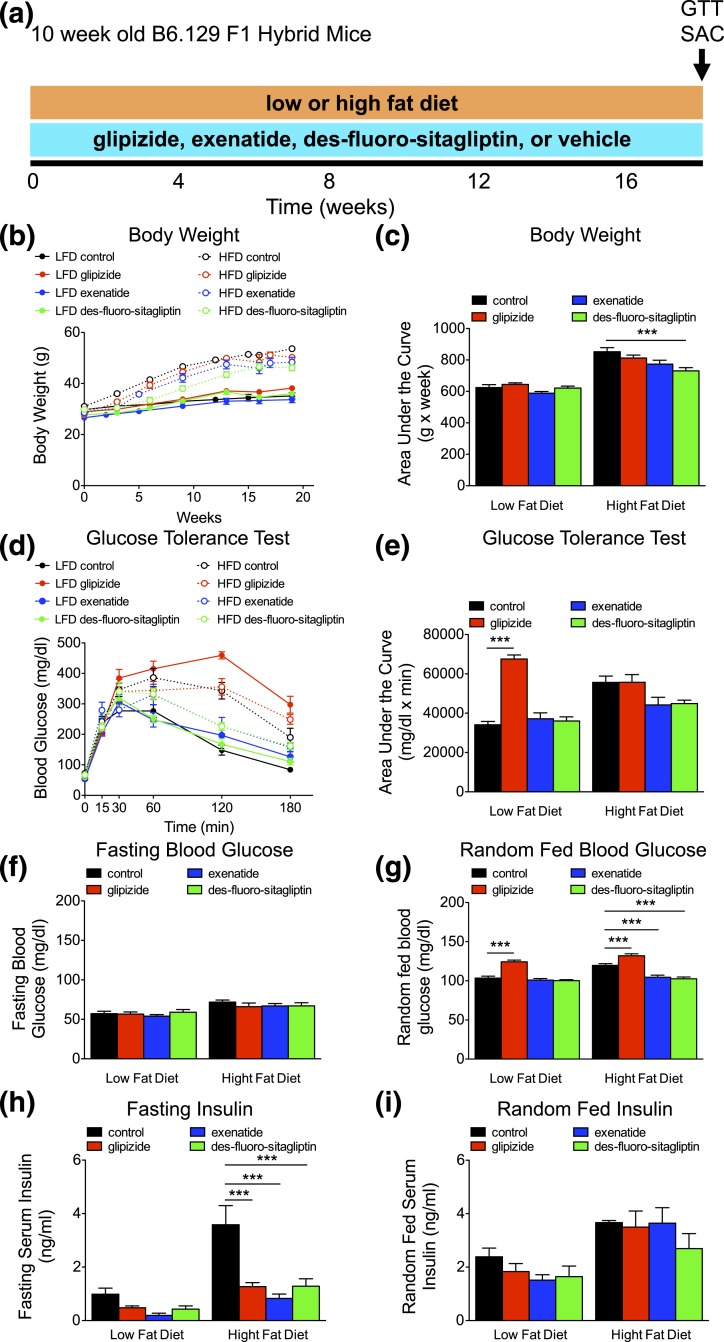
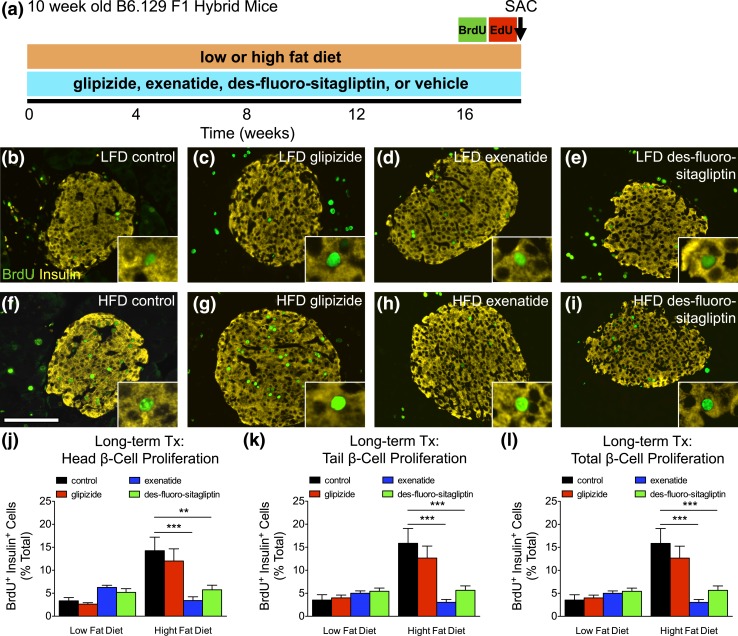
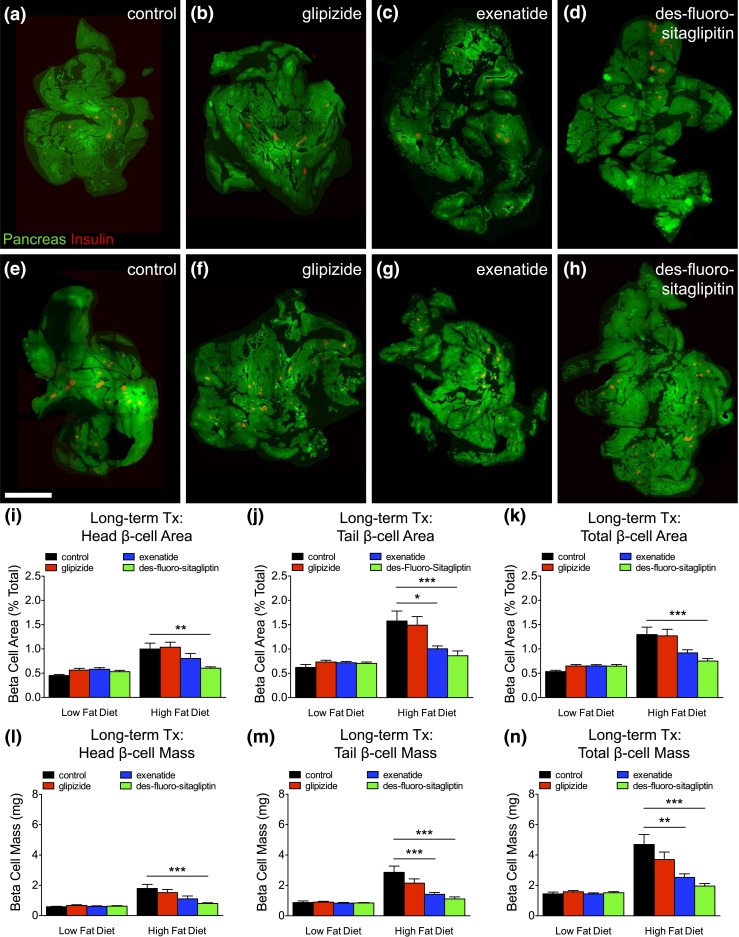
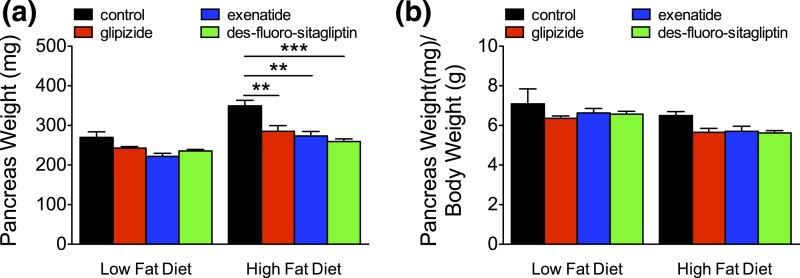
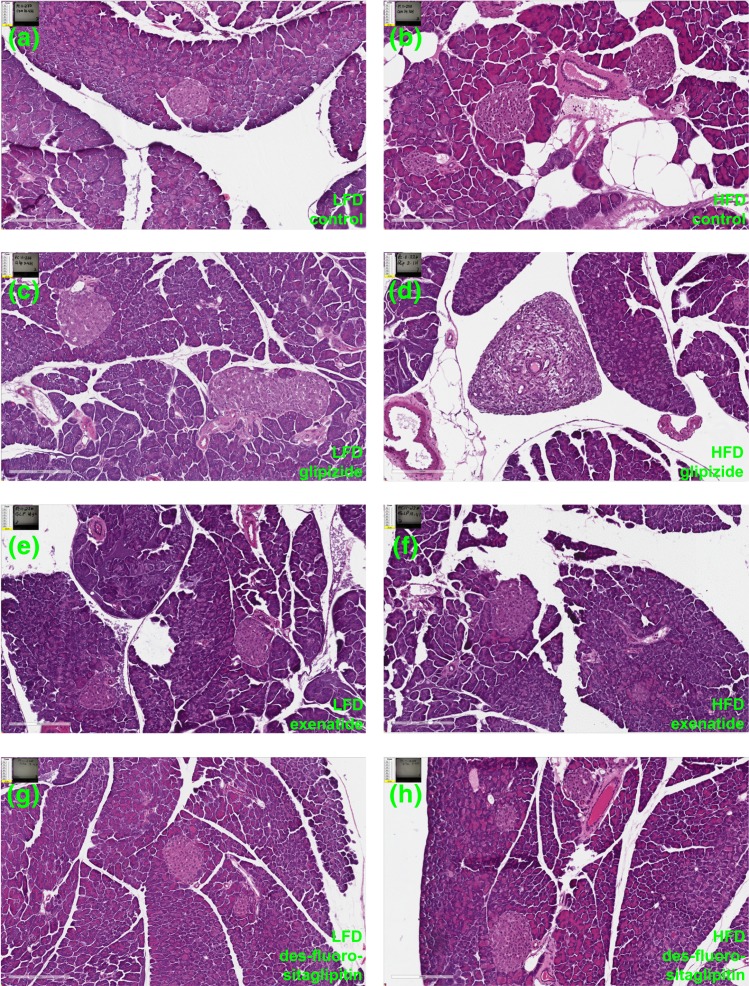
The impact of incretins upon pancreatic β-cell expansion remains extremely controversial. Multiple studies indicate that incretin-based therapies can increase β-cell proliferation, and incretins have been hypothesized to expand β-cell mass. However, disagreement exists on whether incretins increase β-cell mass. Moreover, some reports indicate that incretins may cause metaplastic changes in pancreatic histology. To resolve these questions, we treated a large cohort of mice with incretin-based therapies and carried out a rigorous analysis of β-cell turnover and pancreatic histology using high-throughput imaging. Young mice received exenatide via osmotic pump, des-fluoro-sitagliptin, or glipizide compounded in diet for 2 weeks (short-term) on a low-fat diet (LFD) or 4.5 months (long-term) on a LFD or high-fat diet (HFD). Pancreata were quantified for β-cell turnover and mass. Slides were examined for gross anatomical and microscopic changes to exocrine pancreas. Short-term des-fluoro-sitagliptin increased serum insulin and induced modest β-cell proliferation but no change in β-cell mass. Long-term incretin therapy in HFD-fed mice resulted in reduced weight gain, improved glucose homeostasis, and abrogated β-cell mass expansion. No evidence for rapidly dividing progenitor cells was found in islets or pancreatic parenchyma, indicating that incretins do not induce islet neogenesis or pancreatic metaplasia. Contrasting prior reports, we found no evidence of β-cell mass expansion after acute or chronic incretin therapy. Chronic incretin administration was not associated with histological abnormalities in pancreatic parenchyma; mice did not develop tumors, pancreatitis, or ductal hyperplasia. We conclude that incretin therapies do not generate β-cells or alter pancreatic histology in young mice.
Copyright © 2017 Endocrine Society.
Figures
Comment in
-
Incretin-Based Therapies: Revisiting Their Mode of Action.Endocrinology. 2017 Jun 1;158(6):1560-1563. doi: 10.1210/en.2017-00252. Endocrinology. 2017. PMID: 28575434 Free PMC article. No abstract available.
References
-
- Campbell JE, Drucker DJ. Pharmacology, physiology, and mechanisms of incretin hormone action. Cell Metab. 2013;17(6):819–837. - PubMed
-
- Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet. 2006;368(9548):1696–1705. - PubMed
-
- Xu G, Stoffers DA, Habener JF, Bonner-Weir S. Exendin-4 stimulates both beta-cell replication and neogenesis, resulting in increased beta-cell mass and improved glucose tolerance in diabetic rats. Diabetes. 1999;48(12):2270–2276. - PubMed
-
- Buteau J, Spatz ML, Accili D. Transcription factor FoxO1 mediates glucagon-like peptide-1 effects on pancreatic beta-cell mass. Diabetes. 2006;55(5):1190–1196. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
