

Characteristics of Pediatric vs Adult Pheochromocytomas and Paragangliomas
- PMID: 28324046
- PMCID: PMC5460722
- DOI: 10.1210/jc.2016-3829
Characteristics of Pediatric vs Adult Pheochromocytomas and Paragangliomas
Abstract
Context: Pheochromocytomas and paragangliomas (PPGLs) in children are often hereditary and may present with different characteristics compared with adults. Hereditary PPGLs can be separated into cluster 1 and cluster 2 tumors due to mutations impacting hypoxia and kinase receptor signaling pathways, respectively.
Objective: To identify differences in presentation of PPGLs between children and adults.
Design: A retrospective cross-sectional clinical study.
Setting: Seven tertiary medical centers.
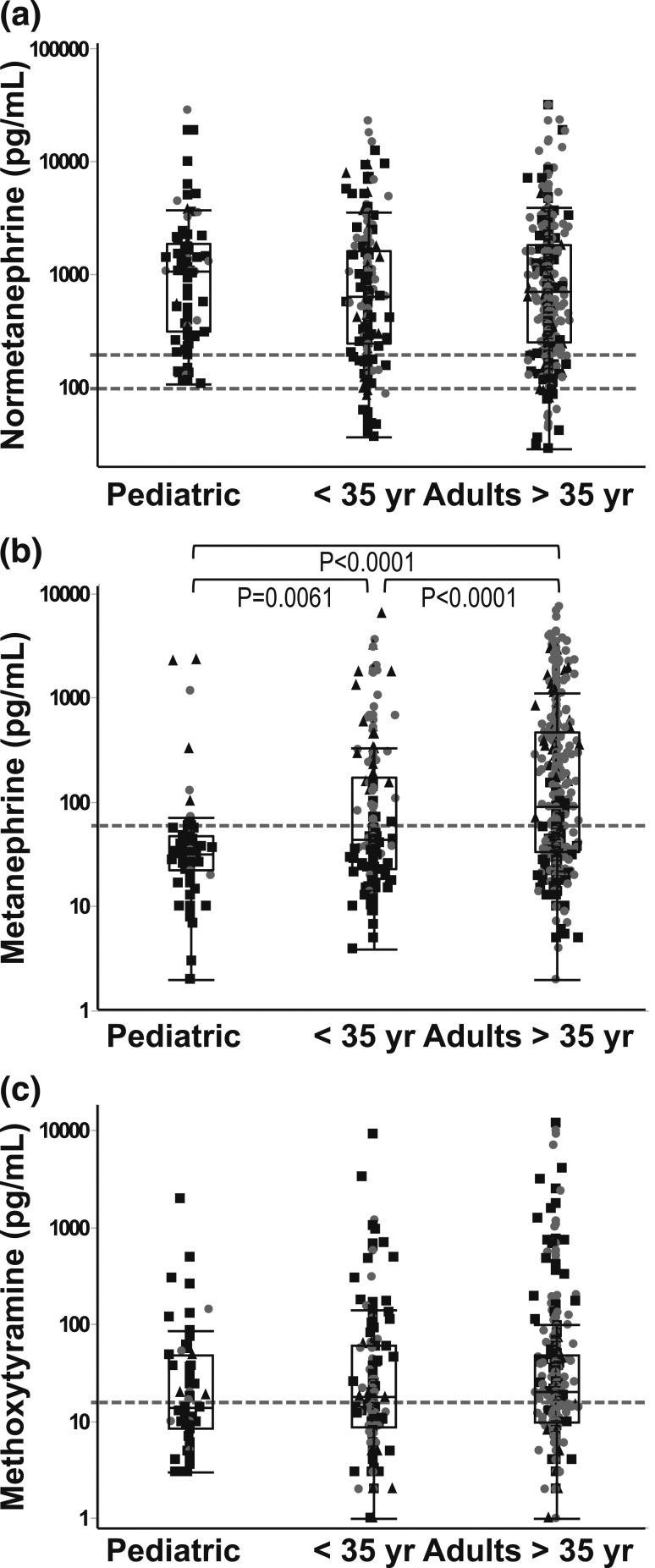
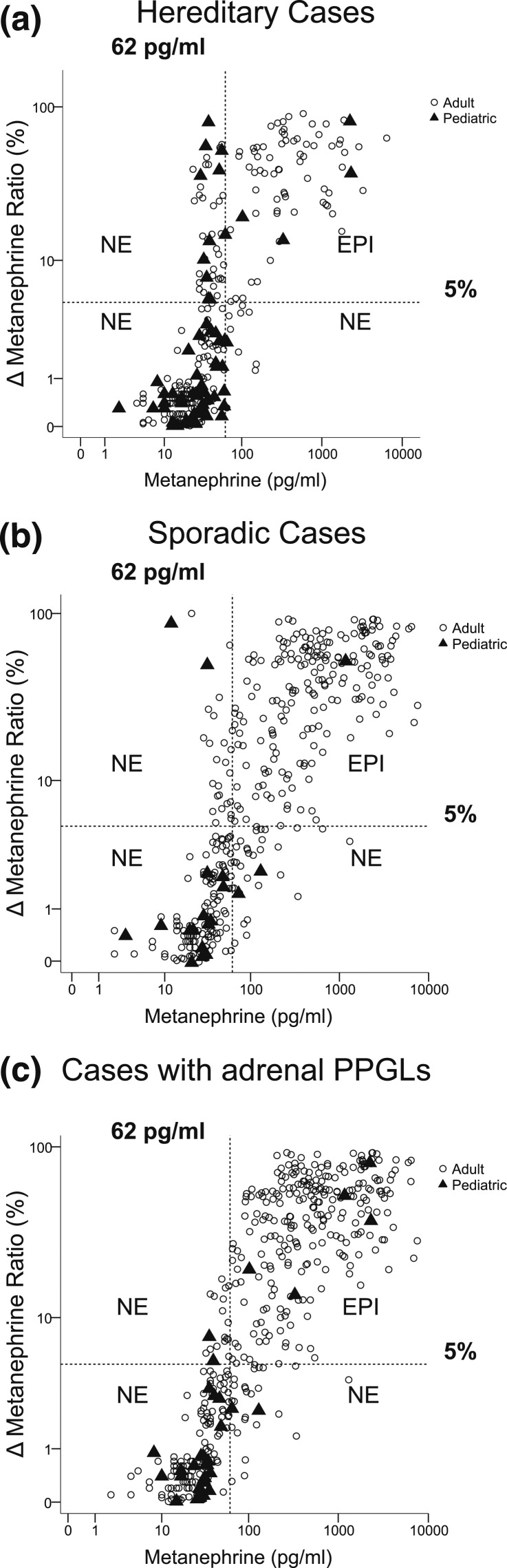
Patients: The study included 748 patients with PPGLs, including 95 with a first presentation during childhood. Genetic testing was available in 611 patients. Other data included locations of primary tumors, presence of recurrent or metastatic disease, and plasma concentrations of metanephrines and 3-methoxytyramine.
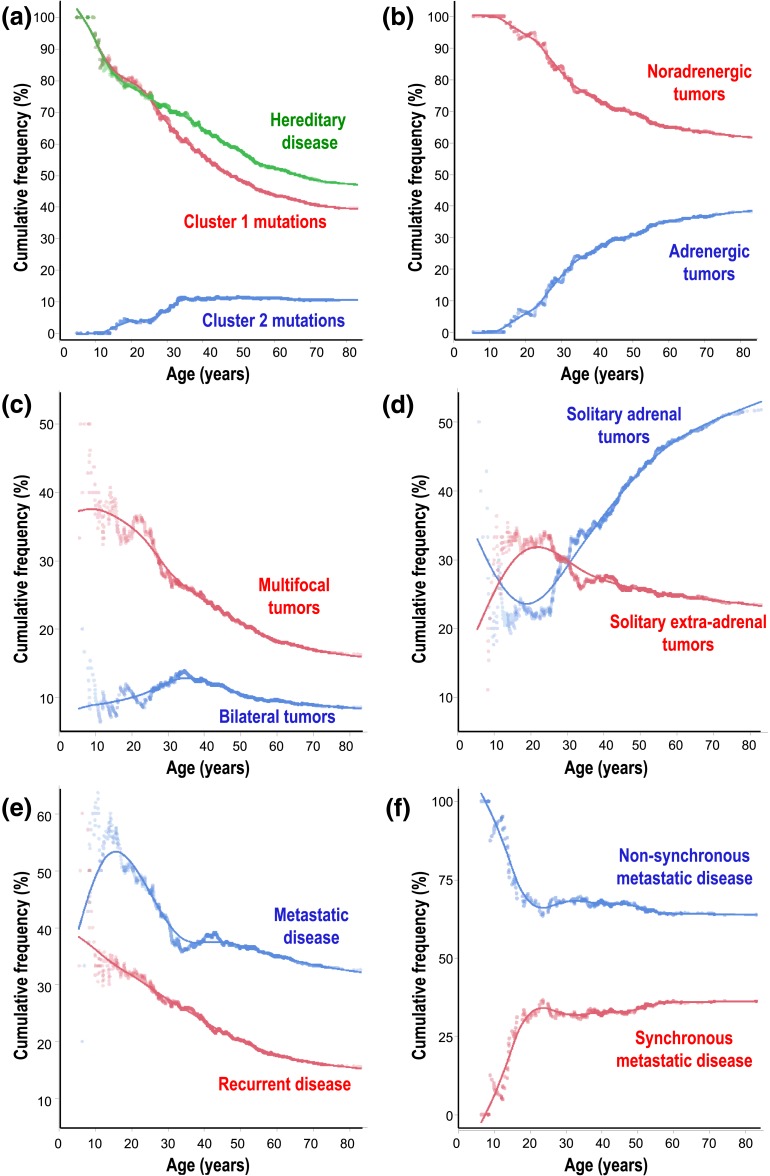
Results: Children showed higher (P < 0.0001) prevalence than adults of hereditary (80.4% vs 52.6%), extra-adrenal (66.3% vs 35.1%), multifocal (32.6% vs 13.5%), metastatic (49.5% vs 29.1%), and recurrent (29.5% vs 14.2%) PPGLs. Tumors due to cluster 1 mutations were more prevalent among children than adults (76.1% vs 39.3%; P < 0.0001), and this paralleled a higher prevalence of noradrenergic tumors, characterized by relative lack of increased plasma metanephrine, in children than in adults (93.2% vs 57.3%; P < 0.0001).
Conclusions: The higher prevalence of hereditary, extra-adrenal, multifocal, and metastatic PPGLs in children than adults represents interrelated features that, in part, reflect the lower age of disease presentation of noradrenergic cluster 1 than adrenergic cluster 2 tumors. The differences in disease presentation are important to consider in children at risk for PPGLs due to a known mutation or previous history of tumor.
Copyright © 2017 by the Endocrine Society
Figures
References
-
- Hume DM. Pheochromocytoma in the adult and in the child. Am J Surg. 1960;99:458–496. - PubMed
-
- Barontini M, Levin G, Sanso G. Characteristics of pheochromocytoma in a 4- to 20-year-old population. Ann N Y Acad Sci. 2006;1073:30–37. - PubMed
-
- Robles JF, Mercado Asis LB, Pacak K. Pheochromocytoma: unmasking the chameleon. In: Koch CA, Chrousos GP, eds. Endocrine Hypertension: Underlying Mechanisms and Therapy. New York, NY: Humana Press; 2012:123–148.
-
- Fonkalsrud EW. Pheochromocytoma in childhood. Prog Pediatr Surg. 1991;26:103–111. - PubMed
-
- Neumann HP, Bausch B, McWhinney SR, Bender BU, Gimm O, Franke G, Schipper J, Klisch J, Altehoefer C, Zerres K, Januszewicz A, Eng C, Smith WM, Munk R, Manz T, Glaesker S, Apel TW, Treier M, Reineke M, Walz MK, Hoang-Vu C, Brauckhoff M, Klein-Franke A, Klose P, Schmidt H, Maier-Woelfle M, Peçzkowska M, Szmigielski C, Eng C; Freiburg-Warsaw-Columbus Pheochromocytoma Study Group . Germ-line mutations in nonsyndromic pheochromocytoma. N Engl J Med. 2002;346(19):1459–1466. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
