

Association Between Radiation Therapy, Surgery, or Observation for Localized Prostate Cancer and Patient-Reported Outcomes After 3 Years
- PMID: 28324093
- PMCID: PMC5782813
- DOI: 10.1001/jama.2017.1704
Association Between Radiation Therapy, Surgery, or Observation for Localized Prostate Cancer and Patient-Reported Outcomes After 3 Years
Erratum in
-
Incorrect Surgery Identified.JAMA. 2017 May 23;317(20):2134. doi: 10.1001/jama.2017.4824. JAMA. 2017. PMID: 28535212 No abstract available.
Abstract
Importance: Understanding the adverse effects of contemporary approaches to localized prostate cancer treatment could inform shared decision making.
Objective: To compare functional outcomes and adverse effects associated with radical prostatectomy, external beam radiation therapy (EBRT), and active surveillance.
Design, setting, and participants: Prospective, population-based, cohort study involving 2550 men (≤80 years) diagnosed in 2011-2012 with clinical stage cT1-2, localized prostate cancer, with prostate-specific antigen levels less than 50 ng/mL, and enrolled within 6 months of diagnosis.
Exposures: Treatment with radical prostatectomy, EBRT, or active surveillance was ascertained within 1 year of diagnosis.
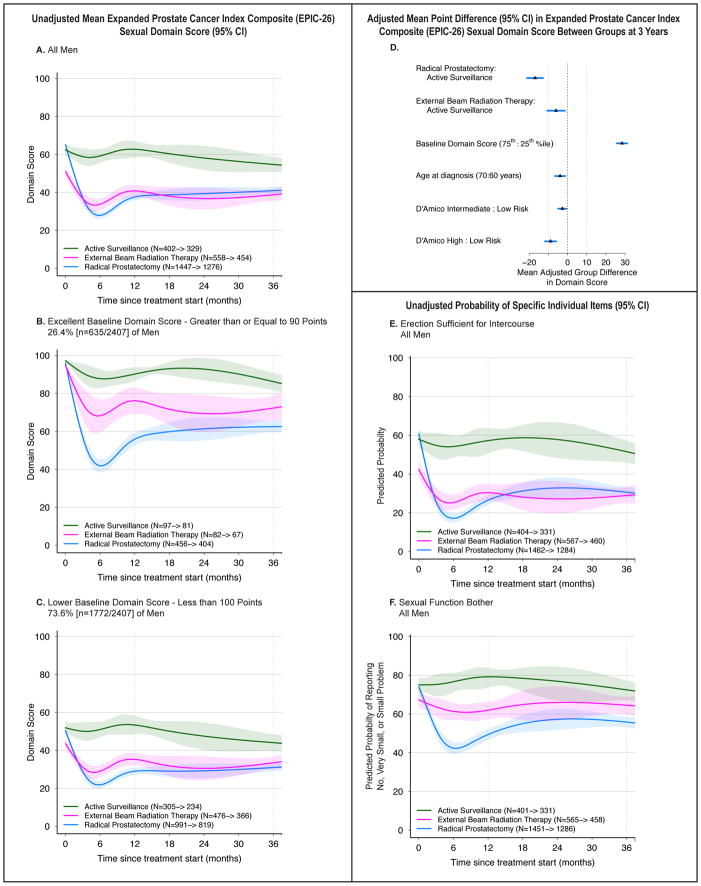
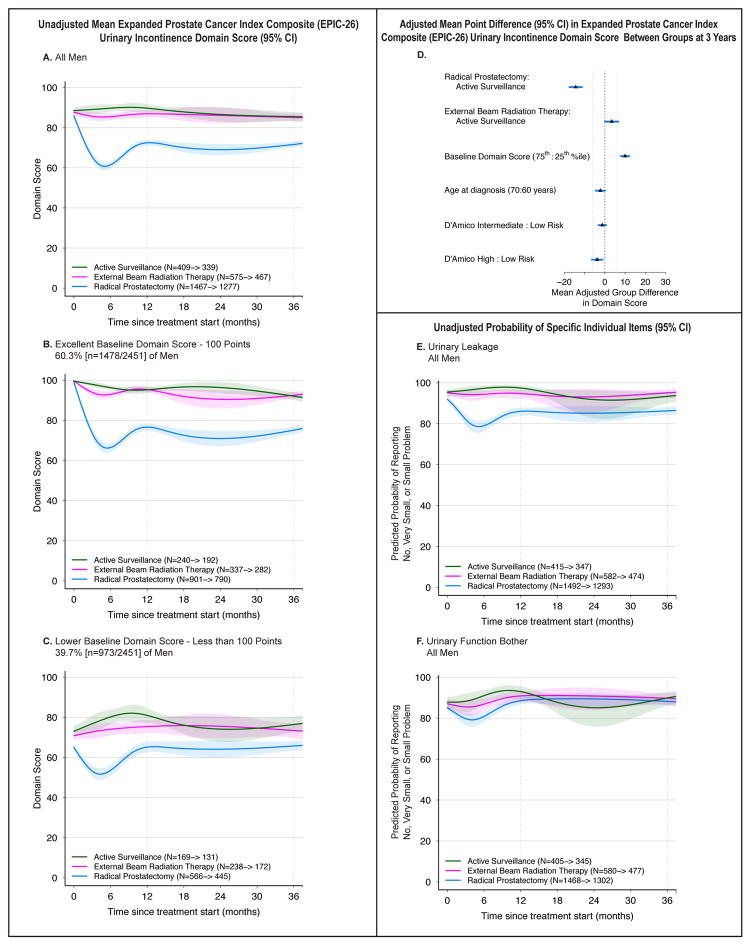
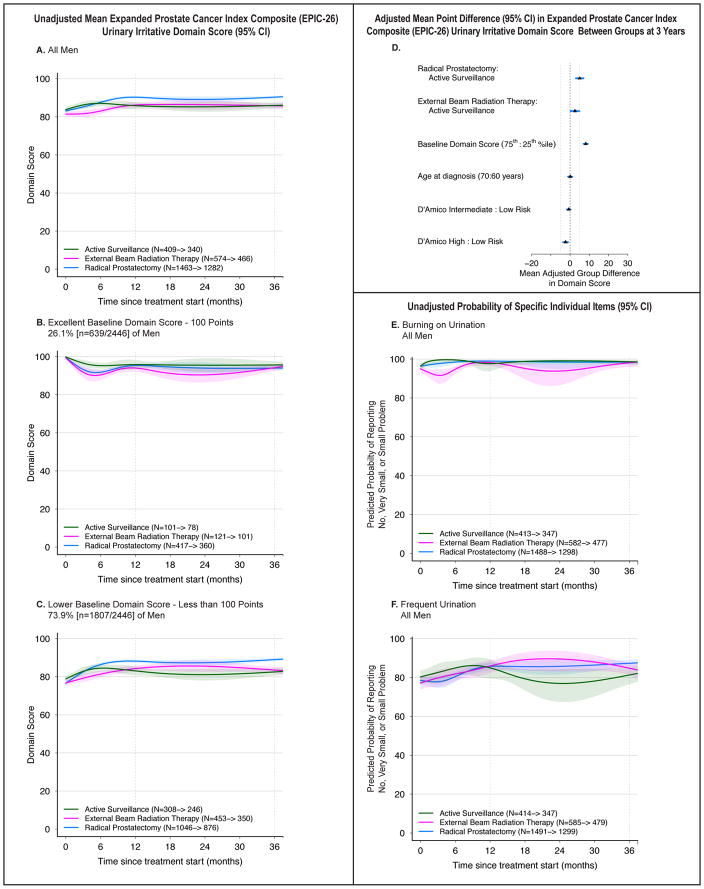
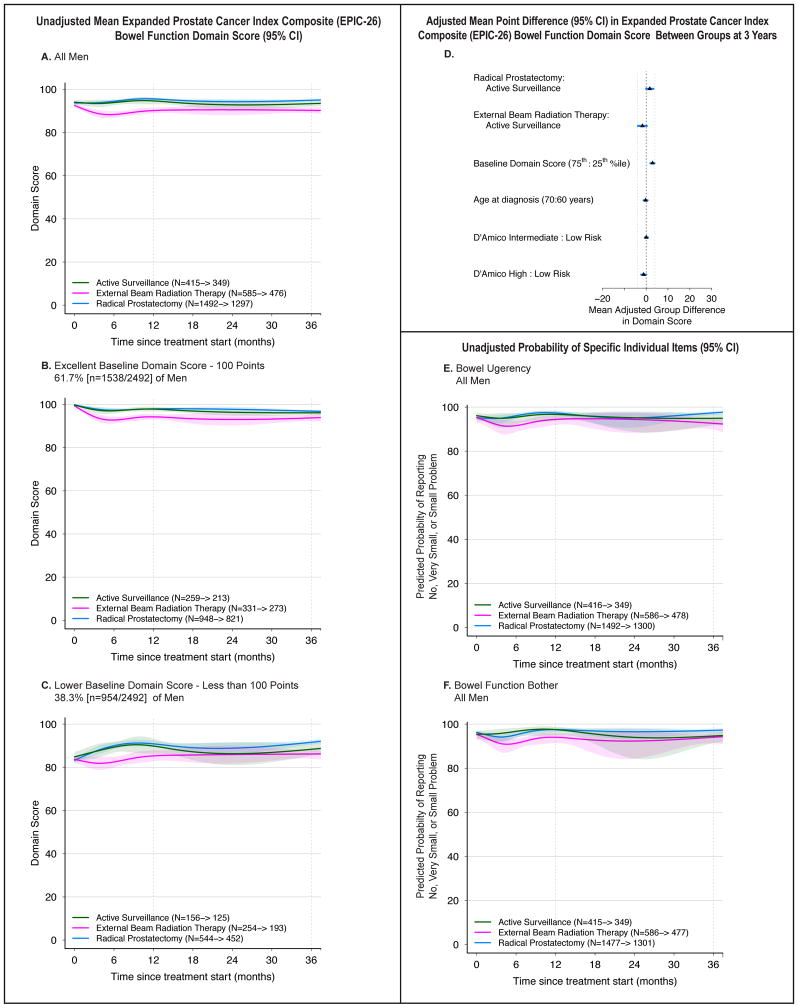
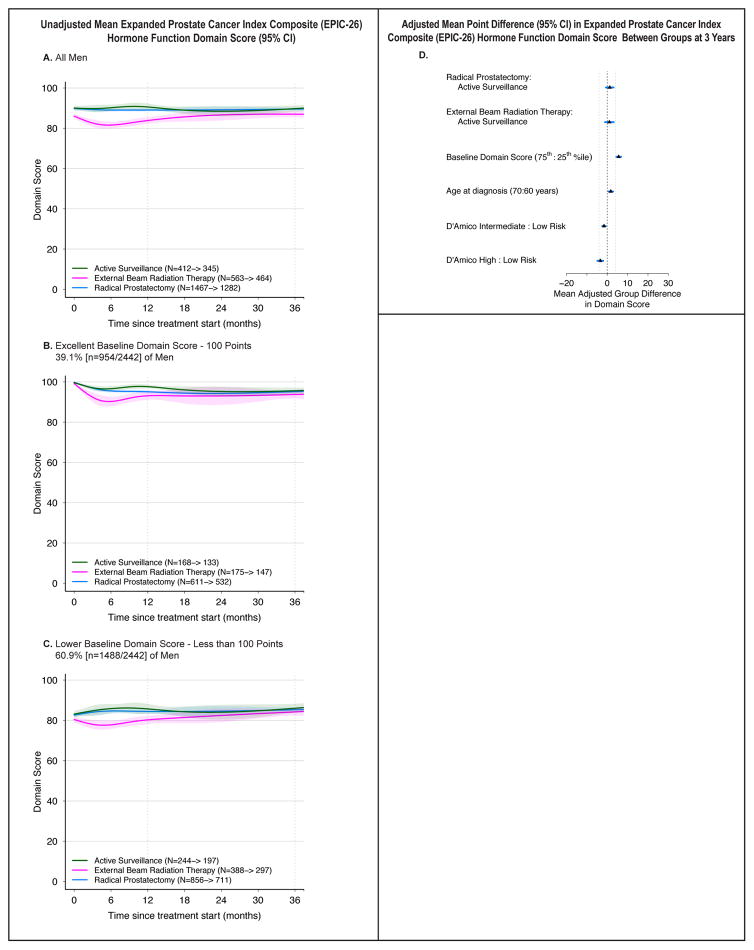
Main outcomes and measures: Patient-reported function on the 26-item Expanded Prostate Cancer Index Composite (EPIC) 36 months after enrollment. Higher domain scores (range, 0-100) indicate better function. Minimum clinically important difference was defined as 10 to 12 points for sexual function, 6 for urinary incontinence, 5 for urinary irritative symptoms, 5 for bowel function, and 4 for hormonal function.
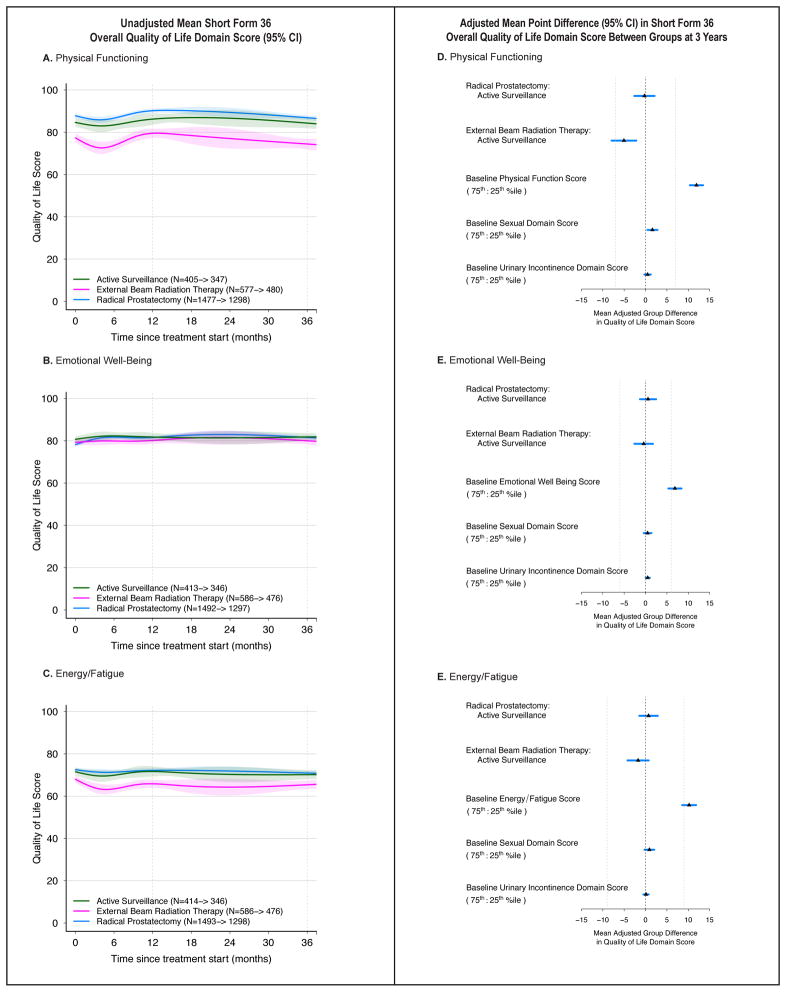
Results: The cohort included 2550 men (mean age, 63.8 years; 74% white, 55% had intermediate- or high-risk disease), of whom 1523 (59.7%) underwent radical prostatectomy, 598 (23.5%) EBRT, and 429 (16.8%) active surveillance. Men in the EBRT group were older (mean age, 68.1 years vs 61.5 years, P < .001) and had worse baseline sexual function (mean score, 52.3 vs 65.2, P < .001) than men in the radical prostatectomy group. At 3 years, the adjusted mean sexual domain score for radical prostatectomy decreased more than for EBRT (mean difference, -11.9 points; 95% CI, -15.1 to -8.7). The decline in sexual domain scores between EBRT and active surveillance was not clinically significant (-4.3 points; 95% CI, -9.2 to 0.7). Radical prostatectomy was associated with worse urinary incontinence than EBRT (-18.0 points; 95% CI, -20.5 to -15.4) and active surveillance (-12.7 points; 95% CI, -16.0 to -9.3) but was associated with better urinary irritative symptoms than active surveillance (5.2 points; 95% CI, 3.2 to 7.2). No clinically significant differences for bowel or hormone function were noted beyond 12 months. No differences in health-related quality of life or disease-specific survival (3 deaths) were noted (99.7%-100%).
Conclusions and relevance: In this cohort of men with localized prostate cancer, radical prostatectomy was associated with a greater decrease in sexual function and urinary incontinence than either EBRT or active surveillance after 3 years and was associated with fewer urinary irritative symptoms than active surveillance; however, no meaningful differences existed in either bowel or hormonal function beyond 12 months or in in other domains of health-related quality-of-life measures. These findings may facilitate counseling regarding the comparative harms of contemporary treatments for prostate cancer.
Figures
Comment in
-
Patient-Reported Outcomes Following Treatment for Localized Prostate Cancer: Helping Decision Making for Patients and Their Physicians.JAMA. 2017 Mar 21;317(11):1121-1123. doi: 10.1001/jama.2017.1703. JAMA. 2017. PMID: 28324073 No abstract available.
-
Prostate cancer: Comparing quality of life outcomes after prostate cancer treatment.Nat Rev Urol. 2017 Jul;14(7):396-397. doi: 10.1038/nrurol.2017.81. Epub 2017 Jun 13. Nat Rev Urol. 2017. PMID: 28607497 No abstract available.
-
You Pays Your Money, You Takes Your Choice: Functional Outcomes Following Curative Treatment for Clinically Localized Prostate Cancer: Commentary on: Association Between Radiation Therapy, Surgery, or Observation for Localized Prostate Cancer and Patient-reported Outcomes After 3 Years.Urology. 2017 Sep;107:3-4. doi: 10.1016/j.urology.2017.06.011. Epub 2017 Jun 15. Urology. 2017. PMID: 28625593 No abstract available.
-
In localised prostate cancer, radical prostatectomy was associated with more sexual dysfunction and urinary incontinence than radiation or active surveillance.Evid Based Med. 2017 Oct;22(5):192. doi: 10.1136/ebmed-2017-110772. Epub 2017 Aug 16. Evid Based Med. 2017. PMID: 28814450 No abstract available.
-
Re: Association between Radiation Therapy, Surgery, or Observation for Localized Prostate Cancer and Patient-Reported Outcomes after 3 Years.J Urol. 2017 Sep;198(3):466-468. doi: 10.1016/j.juro.2017.06.039. Epub 2017 Jun 20. J Urol. 2017. PMID: 28817883 No abstract available.
-
Re: Association between Radiation Therapy, Surgery, or Observation for Localized Prostate Cancer and Patient-Reported Outcomes after 3 Years.J Urol. 2017 Oct;198(4):743-744. doi: 10.1016/j.juro.2017.07.032. Epub 2017 Jul 18. J Urol. 2017. PMID: 28905786 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
