

Multimodality management and outcomes of brain arterio-venous malformations (AVMs) in children: personal experience and review of the literature, with specific emphasis on age at first AVM bleed
- PMID: 28324183
- PMCID: PMC5382178
- DOI: 10.1007/s00381-017-3383-4
Multimodality management and outcomes of brain arterio-venous malformations (AVMs) in children: personal experience and review of the literature, with specific emphasis on age at first AVM bleed
Abstract
Purpose: The purpose of this paper is to study the presentation and analyse the results of multimodality treatment of brain arterio-venous malformations (AVMs) in children at our centre and review age at first AVM rupture in the literature.
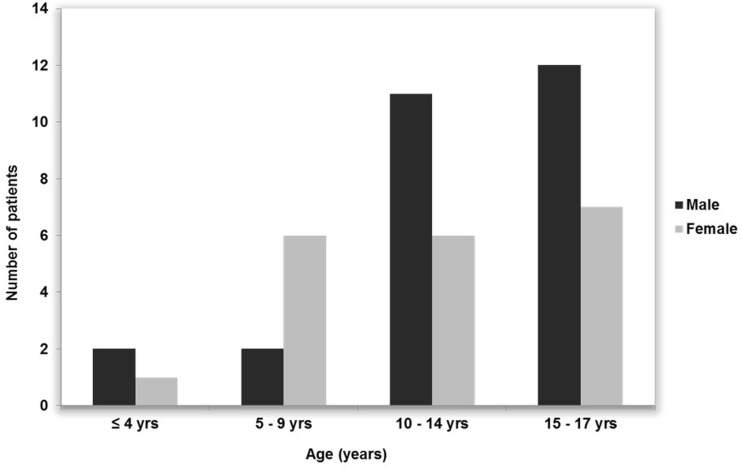
Methods: Of 52 patients aged <18 years, 47 with brain AVMs (27 males and 20 females) aged 4-17 years (mean 12.2) were retrospectively reviewed. PubMed search revealed five additional studies including 267 patients where the prevalence of age-related AVMs rupture was analysed.
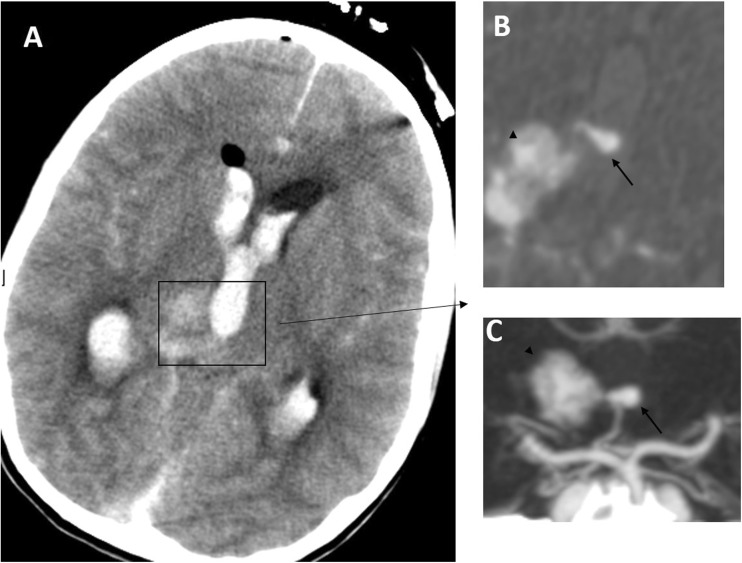
Results: In our study, 37 patients had bled, 9 were symptomatic without haemorrhage and 1 was incidental. Spetzler-Martin score distribution was 5 cases grade I, 18 grade II, 21 grade III and 3 grade IV. Appropriate imaging was performed, either CT/MRI angiogram only (in emergency cases) or catheter angiogram, prior to definitive treatment. There were 40 supratentorial and 7 infratentorial AVMs. Twenty-nine patients had microsurgery alone and 9 patients were treated by radiosurgery only. Three patients were embolised, all followed by radiosurgery, with one requiring surgery too, while 4 patients had combined surgery and radiosurgery. One patient is awaiting radiosurgery while another was not treated. Good outcomes, classified as modified Rankin score (mRS) 0-2 improved significantly after intervention to 89.4% from 38.3% pre-treatment (p value <0.0001). Angiography confirmed 96.6% obliteration after first planned operation. Repeat cerebral angiogram around age 18 was negative in all previously cured patients. Reviewing the literature, 82.0% (95% CI = [77-87]; N = 267) of children diagnosed with brain AVMs (mean age 11.4 ± 0.4) presented with a bleed in the last 22 years. Males significantly outnumbered females (136 vs 84) (p < 0.001). Ninety-five patients underwent surgical intervention alone when compared to other treatment modalities (p < 0.001).
Conclusions: Microsurgical excision of surgically accessible intracranial AVMs remains the primary treatment option with very good outcomes. A significant number of patients' AVMs ruptured around puberty; therefore, understanding the pathophysiology of AVM instability at this age may aid future therapy.
Keywords: DSA; Embolisation; Microsurgery; Outcome; Radiosurgery; Ruptured AVMs.
Conflict of interest statement
The authors have none to declare.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
