

Interspinous implants to treat spinal stenosis
- PMID: 28324328
- PMCID: PMC5435644
- DOI: 10.1007/s12178-017-9413-8
Interspinous implants to treat spinal stenosis
Abstract
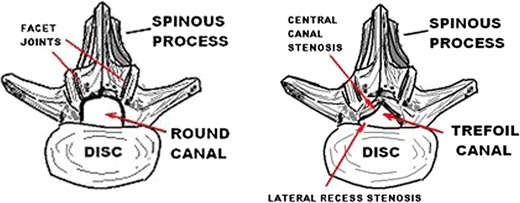
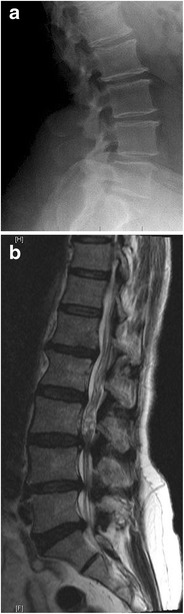
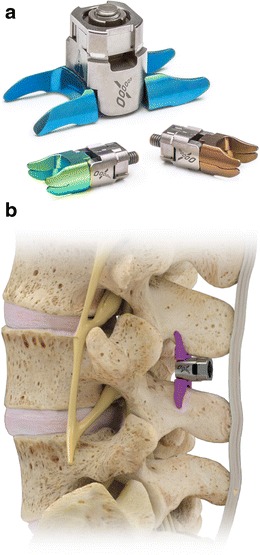
Purpose of review: Lumbar spinal stenosis has historically been treated with open decompressive surgery which is associated with significant morbidity and may give rise to various complications. Interspinous spacers (ISS) have been developed as a less invasive strategy which may serve to avoid many of these risks. The two current spacers that are FDA approved and commercially available are the Coflex and Superion devices. The goal is to review these two implants, their indications, and patient selection.
Recent findings: The Coflex device has been shown to be analogous to decompression and fusion when treating moderate spinal stenosis. It provides dynamic stability after a decompression is performed, without the rigidity of pedicle-screw instrumentation. Recent results show improved outcomes in Coflex patients at 3 years of follow-up, as compared to decompression and fusion. The Superion implant is placed percutaneously in the interspinous space with minimal disruption of spinal anatomy. When compared to the X-Stop device (which is no longer available), the Superion implant shows improved outcomes at 3 years of follow-up. ISS are lesser invasive options as compared to formal decompression and fusion for the treatment of lumbar spinal stenosis.
Keywords: Coflex; Interspinous devices; Interspinous spacers; Lumbar spinal stenosis; Neurogenic claudication; Superion.
Conflict of interest statement
Conflict of interest
Peter G. Whang reports personal fees from Paradigm Spine and institutional support from Vertiflex during the conduct of study.
Raj J. Gala and Glenn S. Russo declare that they have no conflict of interest.
Human and animal rights and informed consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures





References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
