

Smartphone-Based Geofencing to Ascertain Hospitalizations
- PMID: 28325751
- PMCID: PMC5363280
- DOI: 10.1161/CIRCOUTCOMES.116.003326
Smartphone-Based Geofencing to Ascertain Hospitalizations
Abstract
Background: Ascertainment of hospitalizations is critical to assess quality of care and the effectiveness and adverse effects of various therapies. Smartphones, mobile geolocators that are ubiquitous, have not been leveraged to ascertain hospitalizations. Therefore, we evaluated the use of smartphone-based geofencing to track hospitalizations.
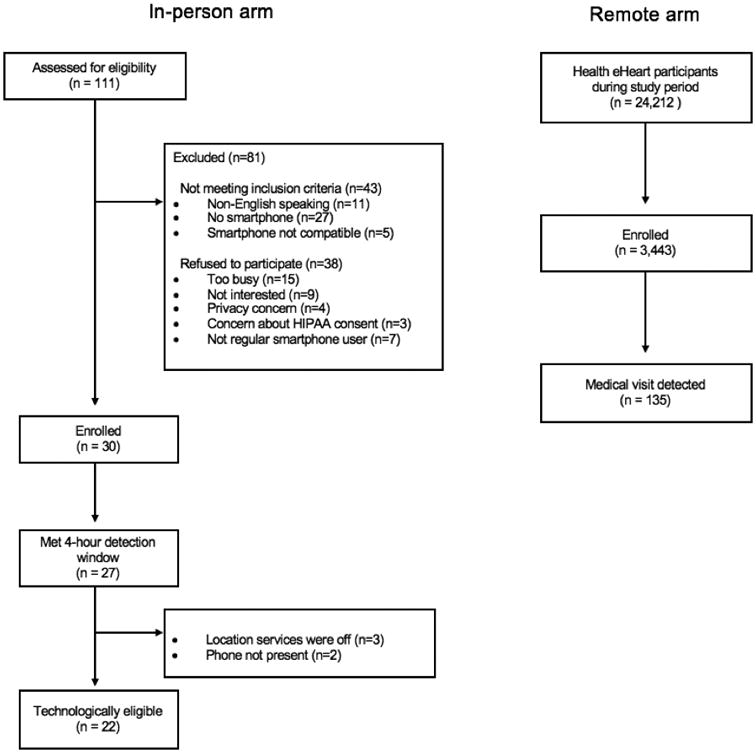
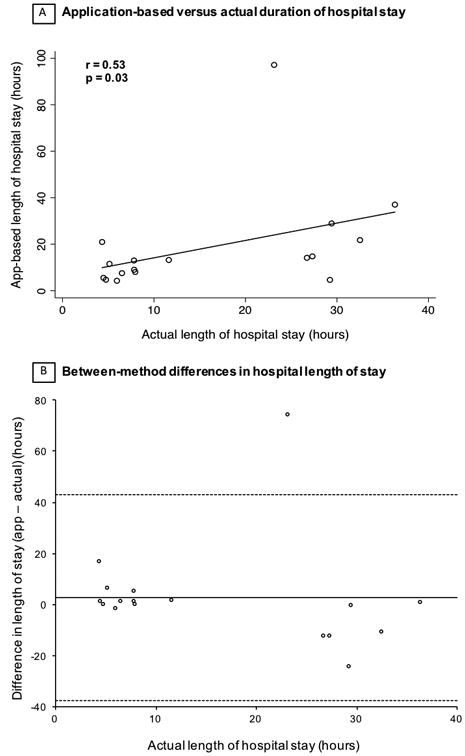
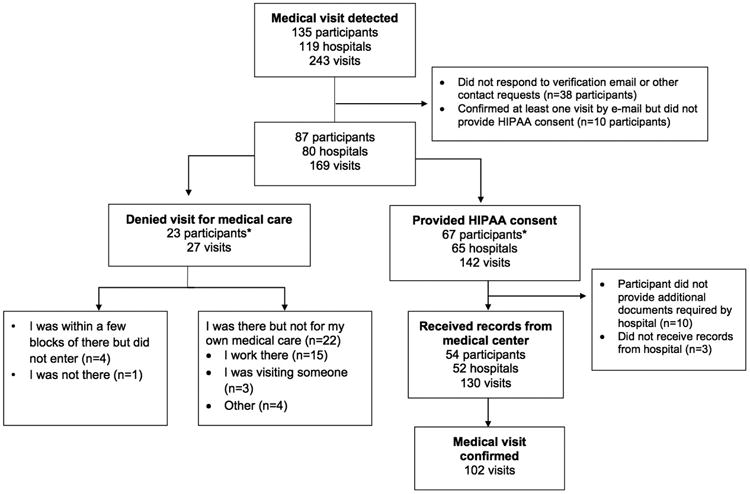
Methods and results: Participants aged ≥18 years installed a mobile application programmed to geofence all hospitals using global positioning systems and cell phone tower triangulation and to trigger a smartphone-based questionnaire when located in a hospital for ≥4 hours. An in-person study included consecutive consenting patients scheduled for electrophysiology and cardiac catheterization procedures. A remote arm invited Health eHeart Study participants who consented and engaged with the study via the internet only. The accuracy of application-detected hospitalizations was confirmed by medical record review as the reference standard. Of 22 eligible in-person patients, 17 hospitalizations were detected (sensitivity 77%; 95% confidence interval, 55%-92%). The length of stay according to the application was positively correlated with the length of stay ascertained via the electronic medical record (r=0.53; P=0.03). In the remote arm, the application was downloaded by 3443 participants residing in all 50 US states; 243 hospital visits at 119 different hospitals were detected through the application. The positive predictive value for an application-reported hospitalization was 65% (95% confidence interval, 57%-72%).
Conclusions: Mobile application-based ascertainment of hospitalizations can be achieved with modest accuracy. This first proof of concept may ultimately be applicable to geofencing other types of prespecified locations to facilitate healthcare research and patient care.
Keywords: fast food; hospitalization; internet; pharmacies; smartphone.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures

Comment in
-
Making Connections: Advancing Healthcare Research Via Consumer Mobile Devices.Circ Cardiovasc Qual Outcomes. 2017 Mar;10(3):e003573. doi: 10.1161/CIRCOUTCOMES.117.003573. Circ Cardiovasc Qual Outcomes. 2017. PMID: 28325752 No abstract available.
References
-
- Hlatky MA, Douglas PS, Cook NL, Wells B, Benjamin EJ, Dickersin K, Goff DC, Hirsch AT, Hylek EM, Peterson ED, Roger VL, Selby JV, Udelson JE, Lauer MS. Future directions for cardiovascular disease comparative effectiveness research: report of a workshop sponsored by the National Heart, Lung, and Blood Institute. J Am Coll Cardiol. 2012;60:569–580. - PMC - PubMed
-
- Heckbert SR, Kooperberg C, Safford MM, Psaty BM, Hsia J, McTiernan A, Gaziano JM, Frishman WH, Curb JD. Comparison of self-report, hospital discharge codes, and adjudication of cardiovascular events in the Women's Health Initiative. Am J Epidemiol. 2004;160:1152–1158. - PubMed
-
- Mell MW, Pettinger M, Proulx-Burns L, Heckbert SR, Allison MA, Criqui MH, Hlatky MA, Burwen DR, Workgroup WPW. Evaluation of Medicare claims data to ascertain peripheral vascular events in the Women's Health Initiative. J Vasc Surg. 2014;60:98–105. - PubMed
-
- Bhandari A, Wagner T. Self-reported utilization of health care services: improving measurement and accuracy. Med Care Res Rev. 2006;63:217–235. - PubMed
-
- Kwon L, Long KD, Wan Y, Yu H, Cunningham BT. Medical diagnostics with mobile devices: Comparison of intrinsic and extrinsic sensing. Biotechnol Adv. 2016;34:291–304. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
