

Exploring why a complex intervention piloted in general practices did not result in an increase in chlamydia screening and diagnosis: a qualitative evaluation using the fidelity of implementation model
- PMID: 28327096
- PMCID: PMC5361828
- DOI: 10.1186/s12875-017-0618-0
Exploring why a complex intervention piloted in general practices did not result in an increase in chlamydia screening and diagnosis: a qualitative evaluation using the fidelity of implementation model
Abstract
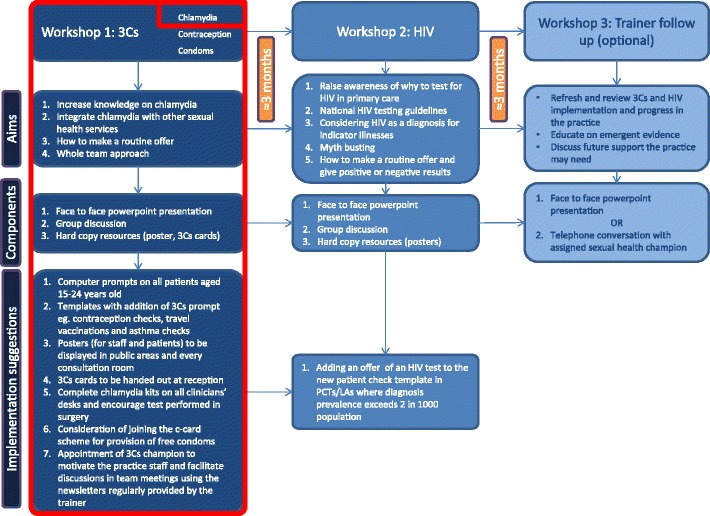
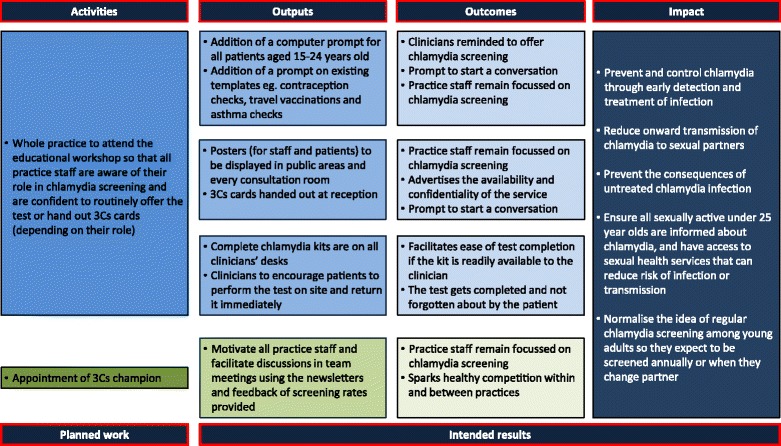
Background: Chlamydia trachomatis (chlamydia) is the most commonly diagnosed sexually transmitted infection (STI) in England; approximately 70% of diagnoses are in sexually active young adults aged under 25. To facilitate opportunistic chlamydia screening in general practice, a complex intervention, based on a previously successful Chlamydia Intervention Randomised Trial (CIRT), was piloted in England. The modified intervention (3Cs and HIV) aimed to encourage general practice staff to routinely offer chlamydia testing to all 15-24 year olds regardless of the type of consultation. However, when the 3Cs (chlamydia screening, signposting to contraceptive services, free condoms) and HIV was offered to a large number of general practitioner (GP) surgeries across England, chlamydia screening was not significantly increased. This qualitative evaluation addresses the following aims: a) Explore why the modified intervention did not increase screening across all general practices. b) Suggest recommendations for future intervention implementation.
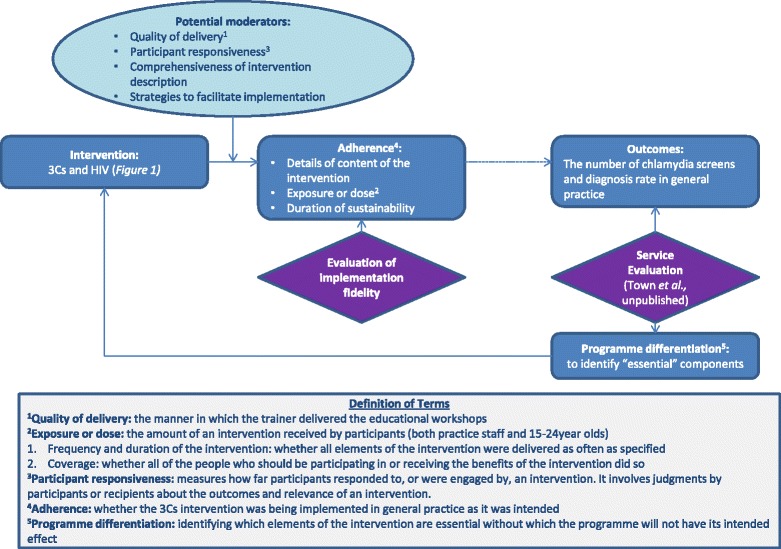
Methods: Phone interviews were carried out with 26 practice staff, at least 5 months after their initial educational workshop, exploring their opinions on the workshop and intervention implementation in the real world setting. Interview transcripts were thematically analysed and further examined using the fidelity of implementation model.
Results: Participants who attended had a positive attitude towards the workshops, but attendee numbers were low. Often, the intervention content, as detailed in the educational workshops, was not adhered to: practice staff were unaware of any on-going trainer support; computer prompts were only added to the female contraception template; patients were not encouraged to complete the test immediately; complete chlamydia kits were not always readily available to the clinicians; and videos and posters were not utilised. Staff reported that financial incentives, themselves, were not a motivator; competing priorities and time were identified as major barriers.
Conclusion: Not adhering to the exact intervention model may explain the lack of significant increases in chlamydia screening. To increase fidelity of implementation outside of Randomised Controlled Trial (RCT) conditions, and consequently, improve likelihood of increased screening, future public health interventions in general practices need to have: more specific action planning within the educational workshop; computer prompts added to systems and used; all staff attending the workshop; and on-going practice staff support with feedback of progress on screening and diagnosis rates fed back to all staff.
Keywords: Adherence; Chlamydia; Educational intervention; Evaluation; Fidelity; General practice; Implementation; Qualitative; Testing; Training.
Figures
References
-
- Public Health England . Sexually transmitted infections and chlamydia screening in England, 2014. 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
