

Allopurinol and the risk of ventricular arrhythmias in the elderly: a study using US Medicare data
- PMID: 28327188
- PMCID: PMC5361697
- DOI: 10.1186/s12916-017-0816-6
Allopurinol and the risk of ventricular arrhythmias in the elderly: a study using US Medicare data
Abstract
Background: There are no published human studies investigating whether the use of allopurinol, the most commonly used medication for the treatment of hyperuricemia in gout, the most common type of inflammatory arthritis in adults, has any beneficial effects on ventricular electrophysiology. The objective of our study was to assess whether allopurinol use is associated with a reduction in the risk of ventricular arrhythmias (VA).
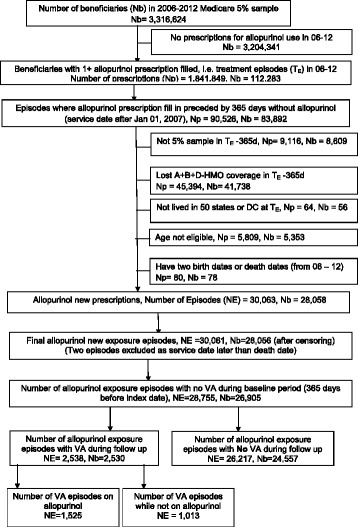
Methods: We used the 5% random sample of Medicare beneficiaries from 2006-2012 to examine new allopurinol use and the risk of incident VA. Multivariable Cox regression analyses were adjusted for demographics (age, race, sex), comorbidity, cardiac medications, and conditions associated with VA. We calculated hazard ratios (HR) and 95% confidence intervals (CI).
Results: Of the 28,755 episodes of new allopurinol use, 2538 were associated with incident VA (8.8%). Among patients with incident VA, 54% were male, 78% were White, 75% had gout as the underlying diagnosis, and the mean Charlson-Romano comorbidity score was 4.8. The crude incidence of VA per 1,000,000 person-days declined as the duration of allopurinol use increased: 1-180 days, 151; 181 days to 2 years, 105; and > 2 years, 85. In multivariable-adjusted analyses, compared to non-use, allopurinol use was associated with lower HR of VA of 0.82 (95% CI, 0.76-0.90). Compared to allopurinol non-use, longer allopurinol use durations were significantly associated with lower multivariable-adjusted HR for VA: 1-180 days, 0.96 (95% CI, 0.85-1.08); 181 days to 2 years, 0.76 (95% CI, 0.68-0.85); and > 2 years, 0.72 (95% CI, 0.60-0.87). Multiple sensitivity analyses adjusting for cardiac conditions, anti-arrhythmic drugs and alternate definitions confirmed our findings with minimal/no attenuation of estimates.
Conclusion: Allopurinol use and use duration of more than 6 months were independently associated with a lower risk of VA. Future studies need to assess the pathophysiology of this potential benefit.
Keywords: Allopurinol; Elderly; Medicare; Risk factor; Ventricular arrhythmias.
Figures

Similar articles
-
The association of gout with incident giant cell arteritis in older adults.Joint Bone Spine. 2019 Mar;86(2):219-224. doi: 10.1016/j.jbspin.2018.05.011. Epub 2018 Jun 7. Joint Bone Spine. 2019. PMID: 29885976
-
Allopurinol and the risk of incident peripheral arterial disease in the elderly: a US Medicare claims data study.Rheumatology (Oxford). 2018 Mar 1;57(3):451-461. doi: 10.1093/rheumatology/kex232. Rheumatology (Oxford). 2018. PMID: 29106674
-
Gout and dementia in the elderly: a cohort study of Medicare claims.BMC Geriatr. 2018 Nov 14;18(1):281. doi: 10.1186/s12877-018-0975-0. BMC Geriatr. 2018. PMID: 30428833 Free PMC article.
-
Managing gout: there's more we can do.J Fam Pract. 2014 Dec;63(12):707-13. J Fam Pract. 2014. PMID: 25486309 Review. No abstract available.
-
Crystal-associated arthritis in the elderly.Rheum Dis Clin North Am. 2007 Feb;33(1):33-55. doi: 10.1016/j.rdc.2006.12.007. Rheum Dis Clin North Am. 2007. PMID: 17367691 Review.
Cited by
-
New Perspectives in Rheumatology: Implications of the Cardiovascular Safety of Febuxostat and Allopurinol in Patients With Gout and Cardiovascular Morbidities Trial and the Associated Food and Drug Administration Public Safety Alert.Arthritis Rheumatol. 2018 Nov;70(11):1702-1709. doi: 10.1002/art.40583. Arthritis Rheumatol. 2018. PMID: 29869840 Free PMC article.
-
Assessment of Cardiovascular Risk in Older Patients With Gout Initiating Febuxostat Versus Allopurinol: Population-Based Cohort Study.Circulation. 2018 Sep 11;138(11):1116-1126. doi: 10.1161/CIRCULATIONAHA.118.033992. Circulation. 2018. PMID: 29899013 Free PMC article.
-
Hyperuricemia is associated with an increased prevalence of ventricular tachycardia and fibrillation in patients with ST-elevation myocardial infarction after primary percutaneous coronary intervention.BMC Cardiovasc Disord. 2022 Apr 26;22(1):199. doi: 10.1186/s12872-022-02635-4. BMC Cardiovasc Disord. 2022. PMID: 35473480 Free PMC article.
-
Effects of Allopurinol on Endothelial Function: A Systematic Review and Meta-Analysis of Randomized Placebo-Controlled Trials.Drugs. 2018 Jan;78(1):99-109. doi: 10.1007/s40265-017-0839-5. Drugs. 2018. PMID: 29139092
-
Promising effects of xanthine oxidase inhibition by allopurinol on autonomic heart regulation estimated by heart rate variability (HRV) analysis in rats exposed to hypoxia and hyperoxia.PLoS One. 2018 Feb 12;13(2):e0192781. doi: 10.1371/journal.pone.0192781. eCollection 2018. PLoS One. 2018. PMID: 29432445 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
