

Combined methylmalonic acidemia and homocysteinemia presenting predominantly with late-onset diffuse lung disease: a case series of four patients
- PMID: 28327205
- PMCID: PMC5360033
- DOI: 10.1186/s13023-017-0610-8
Combined methylmalonic acidemia and homocysteinemia presenting predominantly with late-onset diffuse lung disease: a case series of four patients
Abstract
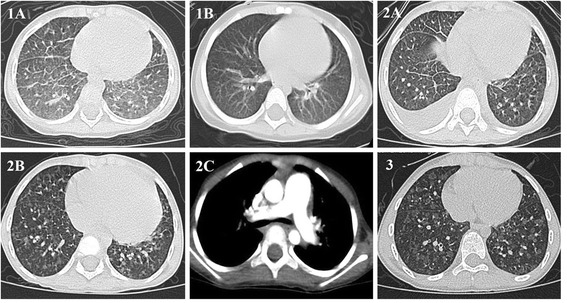
Combined methylmalonic acidemia (MMA) and homocysteinemia are a group of autosomal recessive disorders caused by inborn errors of cobalamin metabolism, including CblC, D, F, and J, with cblC being the most common subtype. The clinical manifestations of combined MMA and homocysteinemia vary, but typically include neurologic, developmental and hematologic abnormalities.We report 4 children with combined MMA and homocysteinemia who presented predominantly with late-onset diffuse lung diseases (DLD). Of these, 3 accompanied by pulmonary arterial hypertension (PAH), 1 accompanied by hypertension, and 2 accompanied by renal thrombotic microangiopathy (TMA), which was confirmed by renal biopsy. This confirms combined MMA and homocysteinemia should be considered in the differential diagnosis of DLD with or without PAH or renal TMA.
Keywords: Children; Diffuse Lung disease; Homocysteinemia; Homocystinuria; Hypertension arterial pulmonary; Methylmalonic acidemia.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
