

Neurocognitive dysfunction in HIV-infected youth: investigating the relationship with immune activation
- PMID: 28327462
- PMCID: PMC5940002
- DOI: 10.3851/IMP3157
Neurocognitive dysfunction in HIV-infected youth: investigating the relationship with immune activation
Abstract
Background: HIV-infected individuals are at increased risk of neurocognitive impairment compared to the general population. Studies suggest that, despite combination antiretroviral therapy (cART), HIV infection causes immune activation which results in neural damage; however, few data exist in HIV-infected youth.
Methods: HIV-infected youth 8-26-years-old on cART with virological suppression were prospectively enrolled along with healthy controls. Neurocognitive performance was assessed by age-appropriate Wechsler Intelligence Scales. Soluble and cellular markers of T-lymphocyte and monocyte activation were measured by ELISA and flow cytometry, respectively.
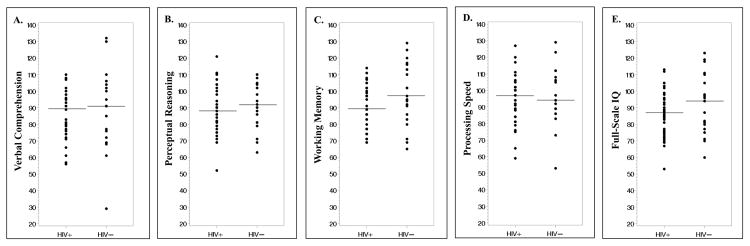
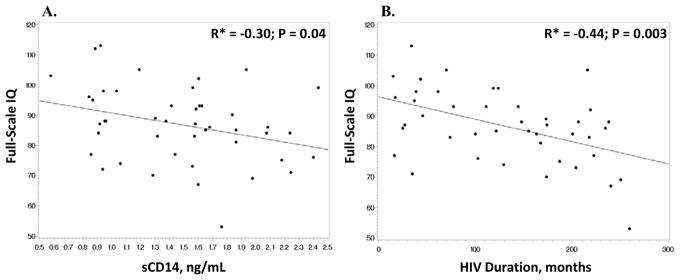
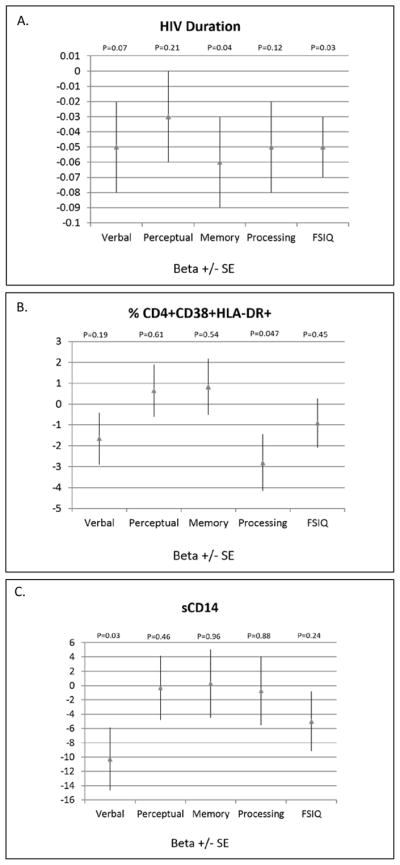
Results: 45 HIV-infected subjects and 21 controls were enrolled. Markers of T-cell and monocyte activation were higher in the HIV-infected subjects compared to controls, but proportions of inflammatory and patrolling monocytes were similar. Although there were no significant differences in neurocognitive scores between the HIV-infected and control groups, scores were low-average for four of five testing domains for the HIV-infected subjects and average for all five in the controls, and % of HIV-infected subjects with scores classified as 'low average' or below was higher than in the controls. Variables most associated with neurocognitive performance among HIV-infected subjects included activated CD4+ T-cells (% CD4+CD38+HLA-DR), monocyte activation (soluble CD14), HIV duration, age and sex.
Conclusions: HIV-infected youth on cART with virological suppression show subtle evidence of neurocognitive impairment compared to healthy controls, and increased immune activation appears to play a role. Additional studies are needed to develop strategic interventions beyond cART to potentially improve neurocognitive performance and/or minimize further impairment in this vulnerable population. ClinicalTrials.gov Identifier: NCT01523496.
Conflict of interest statement
Figures
References
-
- Van Rie AHP, Dow A, Robertson K. Neurologic and neurodevelopmental manifestations of pediatric HIV/AIDS: A global perspective. European journal of paediatric neurology : EJPN : official journal of the European Paediatric Neurology Society. 2007;11:1–9. - PubMed
-
- Schouten J, Cinque P, Gisslen M, Reiss P, Portegies P. HIV-1 infection and cognitive impairment in the cART era: a review. Aids. 2011 Mar 13;25(5):561–575. - PubMed
-
- Drotar D, Olness K, Wiznitzer M, et al. Neurodevelopmental outcomes of Ugandan infants with HIV infection: an application of growth curve analysis. Health Psychol. 1999 Mar;18(2):114–121. - PubMed
-
- Gay CL, Armstrong FD, Cohen D, et al. The effects of HIV on cognitive and motor development in children born to HIV-seropositive women with no reported drug use: birth to 24 months. Pediatrics. 1995 Dec;96(6):1078–1082. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
