

Magnetic Resonance Imaging in the Prognostic Evaluation of Patients with Pulmonary Arterial Hypertension
- PMID: 28328237
- PMCID: PMC5519970
- DOI: 10.1164/rccm.201611-2365OC
Magnetic Resonance Imaging in the Prognostic Evaluation of Patients with Pulmonary Arterial Hypertension
Abstract
Rationale: Prognostication is important when counseling patients and defining treatment strategies in pulmonary arterial hypertension (PAH).
Objectives: To determine the value of magnetic resonance imaging (MRI) metrics for prediction of mortality in PAH.
Methods: Consecutive patients with PAH undergoing MRI were identified from the ASPIRE (Assessing the Spectrum of Pulmonary Hypertension Identified at a Referral Centre) pulmonary hypertension registry.
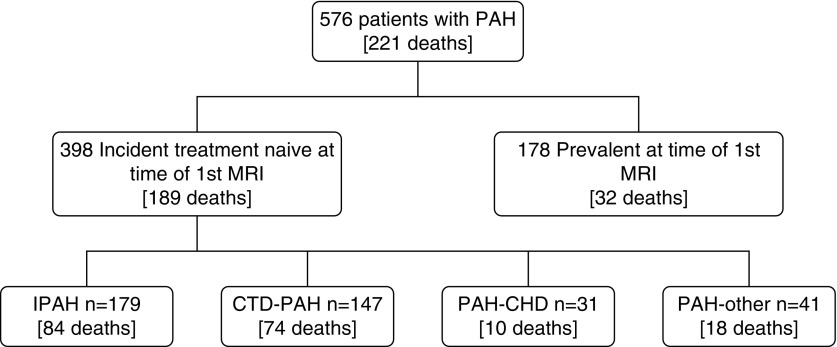
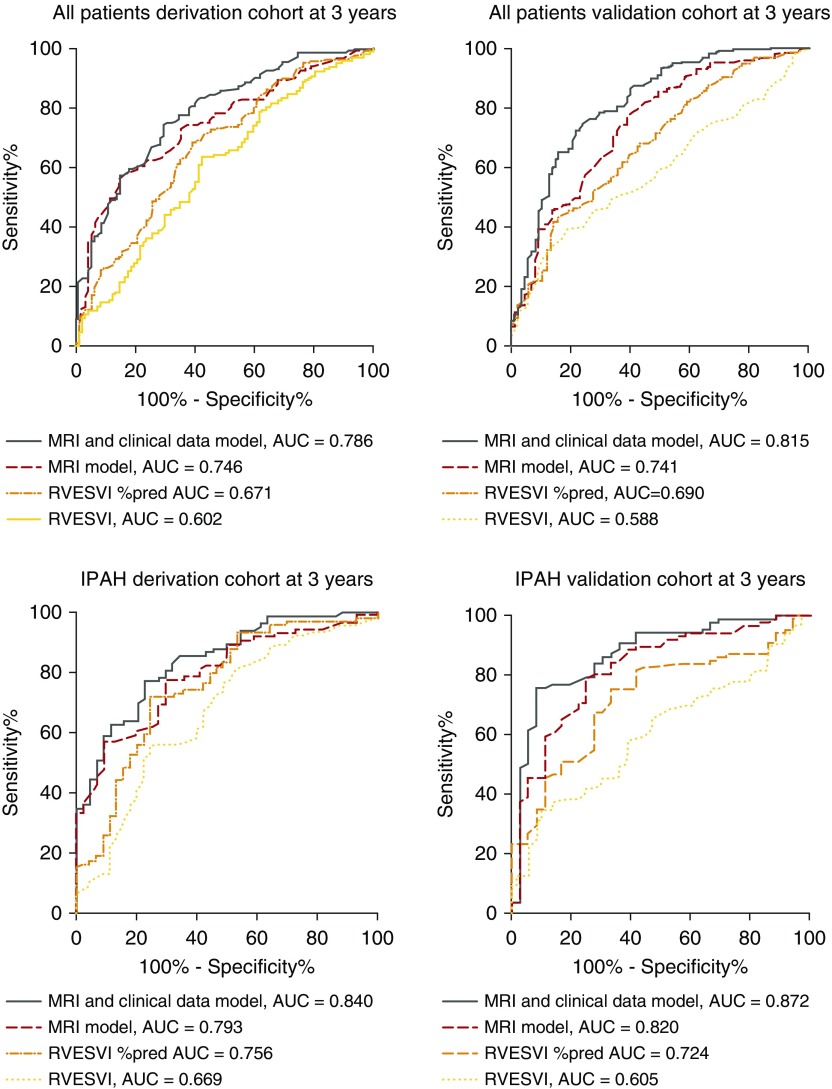
Measurements and main results: During the follow-up period of 42 (range, 17-142) months 576 patients were studied and 221 (38%) died. A derivation cohort (n = 288; 115 deaths) and validation cohort (n = 288; 106 deaths) were identified. We used multivariate Cox regression and found two independent MRI predictors of death (P < 0.01): right ventricular end-systolic volume index adjusted for age and sex, and the relative area change of the pulmonary artery. A model of MRI and clinical data constructed from the derivation cohort predicted mortality in the validation cohort at 1 year (sensitivity, 70 [95% confidence interval (CI), 53-83]; specificity, 62 [95% CI, 62-68]; positive predictive value [PPV], 24 [95% CI, 16-32]; negative predictive value [NPV], 92 [95% CI, 87-96]) and at 3 years (sensitivity, 77 [95% CI, 67-85]; specificity, 73 [95% CI, 66-85]; PPV, 56 [95% CI, 47-65]; and NPV, 87 [95% CI, 81-92]). The model was more accurate in patients with idiopathic PAH at 3 years (sensitivity, 89 [95% CI, 65-84]; specificity, 76 [95% CI, 65-84]; PPV, 60 [95% CI, 46-74]; and NPV, 94 [95% CI, 85-98]).
Conclusions: MRI measurements reflecting right ventricular structure and stiffness of the proximal pulmonary vasculature are independent predictors of outcome in PAH. In combination with clinical data MRI has moderate prognostic accuracy in the evaluation of patients with PAH.
Keywords: magnetic resonance imaging; prognosis; prognostic models; pulmonary arterial hypertension.
Figures

Comment in
-
Magnetic Resonance Imaging in Pulmonary Arterial Hypertension. Panacea or Pixelation?Am J Respir Crit Care Med. 2017 Jul 15;196(2):129-131. doi: 10.1164/rccm.201704-0721ED. Am J Respir Crit Care Med. 2017. PMID: 28707971 No abstract available.
-
Reply to Hou et al.: Can Magnetic Resonance Imaging Effectively Evaluate the Prognosis of Patients with Pulmonary Arterial Hypertension?Am J Respir Crit Care Med. 2018 Mar 1;197(5):676-677. doi: 10.1164/rccm.201709-1842LE. Am J Respir Crit Care Med. 2018. PMID: 28961018 Free PMC article. No abstract available.
-
Can Magnetic Resonance Imaging Effectively Evaluate the Prognosis of Patients with Pulmonary Arterial Hypertension?Am J Respir Crit Care Med. 2018 Mar 1;197(5):675-676. doi: 10.1164/rccm.201707-1530LE. Am J Respir Crit Care Med. 2018. PMID: 28961026 No abstract available.
References
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS) Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37:67–119.
-
- Kiely DG, Elliot CA, Sabroe I, Condliffe R. Pulmonary hypertension: diagnosis and management. BMJ. 2013;346:f2028. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, Frost A, Barst RJ, Badesch DB, Elliott CG, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) Circulation. 2010;122:164–172. - PubMed
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–349. - PubMed
-
- Nickel N, Golpon H, Greer M, Knudsen L, Olsson K, Westerkamp V, Welte T, Hoeper MM. The prognostic impact of follow-up assessments in patients with idiopathic pulmonary arterial hypertension. Eur Respir J. 2012;39:589–596. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
