

Long-term outcomes of surgery alone versus surgery following preoperative chemoradiotherapy for early T3 rectal cancer: A propensity score analysis
- PMID: 28328820
- PMCID: PMC5371457
- DOI: 10.1097/MD.0000000000006362
Long-term outcomes of surgery alone versus surgery following preoperative chemoradiotherapy for early T3 rectal cancer: A propensity score analysis
Abstract
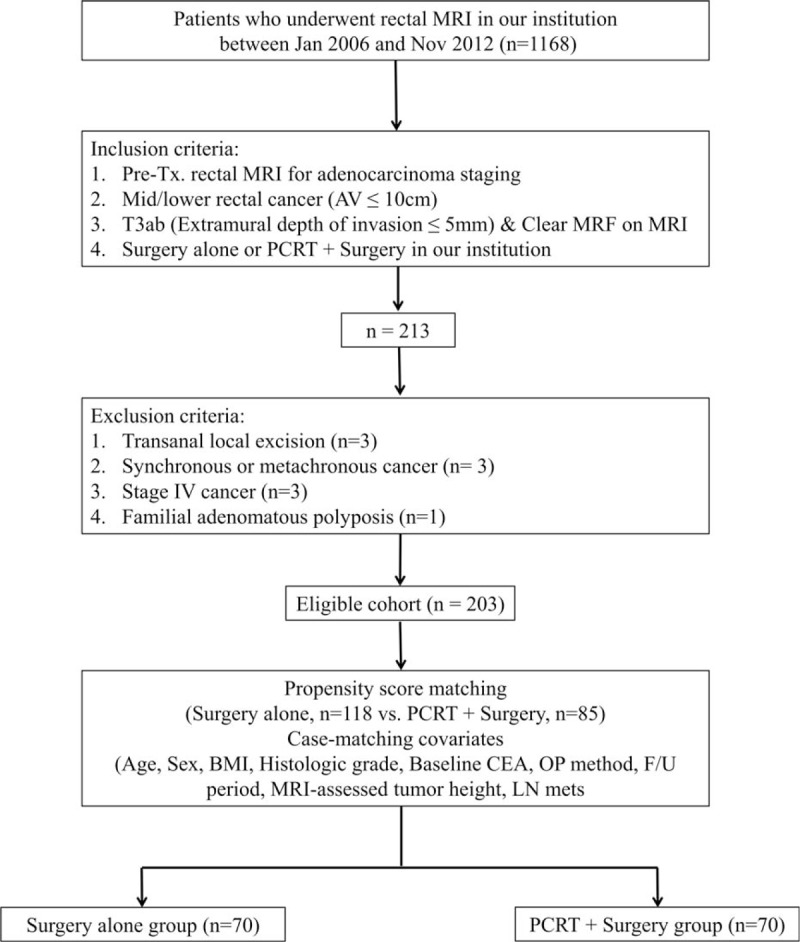
Recently, a few studies have raised the question of whether preoperative chemoradiotherapy (PCRT) is essential for all T3 rectal cancers. This case-matched study aimed to compare the long-term outcomes of surgery alone with those of PCRT + surgery for magnetic resonance imaging (MRI)-assessed T3ab (extramural depth of invasion ≤5 mm) and absent mesorectal fascia invasion (clear MRF) in mid/lower rectal cancer patients.From January 2006 to November 2012, 203 patients who underwent curative surgery alone (n = 118) or PCRT + surgery (n = 85) were enrolled in this retrospective study. A 1:1 propensity score-matched analysis was performed to eliminate the inherent bias. Case-matching covariates included age, sex, body mass index, histologic grade, carcinoembryonic antigen, operation method, follow-up period, tumor height, and status of lymph node metastasis. The end-points were the 5-year local recurrence (LR) rate and disease-free-survival (DFS).After propensity score matching, 140 patients in 70 pairs were included. Neither the 5-year LR rate nor the DFS was significantly different between the 2 groups (the 5-year LR rate, P = 0.93; the 5-year DFS, P = 0.94). The 5-year LR rate of the surgery alone was 2% (95% confidence interval [CI] 0.2%-10.9%) versus 2% (95% CI 0.2%-10.1%) in the PCRT + surgery group. The 5-year DFS of the surgery alone was 87% (95% CI 74.6%-93.7%) versus 88% (95% CI 77.8%-93.9%) in the PCRT + surgery group.In patients with MRI-assessed T3ab and clear MRF mid/lower rectal cancer, the long-term outcomes of surgery alone were comparable with those of the PCRT + surgery. The suggested MRI-assessed T3ab and clear MRF can be used as a highly selective indication of surgery alone in mid/lower T3 rectal cancer. Additionally, in those patients, surgery alone can be tailored to the clinical situation.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

References
-
- NCCN. Practice guideline in diagnosis and treatment of rectal cancer. National Cancer Comprehensive Network, 2013. Available at www.nccn.org.
-
- IKNL Integraal Kankercentrum Nederland. Dutch Guidelines Rectal Cancer, 2011. Available at www.oncoline.nl.
-
- Schmoll HJ, Van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. A personalized approach to clinical decision making. Ann oncol 2012;23:2479–516. - PubMed
-
- NICE. NICE clinical guideline 131. The diagnosis and management of colorectal cancer, 2011. Available at http://guidance. nice.org.uk/cg131.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
