

Coronary Artery Calcification and Risk of Cardiovascular Disease and Death Among Patients With Chronic Kidney Disease
- PMID: 28329057
- PMCID: PMC5798875
- DOI: 10.1001/jamacardio.2017.0363
Coronary Artery Calcification and Risk of Cardiovascular Disease and Death Among Patients With Chronic Kidney Disease
Abstract
Importance: Coronary artery calcification (CAC) is highly prevalent in dialysis-naive patients with chronic kidney disease (CKD). However, there are sparse data on the association of CAC with subsequent risk of cardiovascular disease and all-cause mortality in this population.
Objective: To study the prospective association of CAC with risk of cardiovascular disease and all-cause mortality among dialysis-naive patients with CKD.
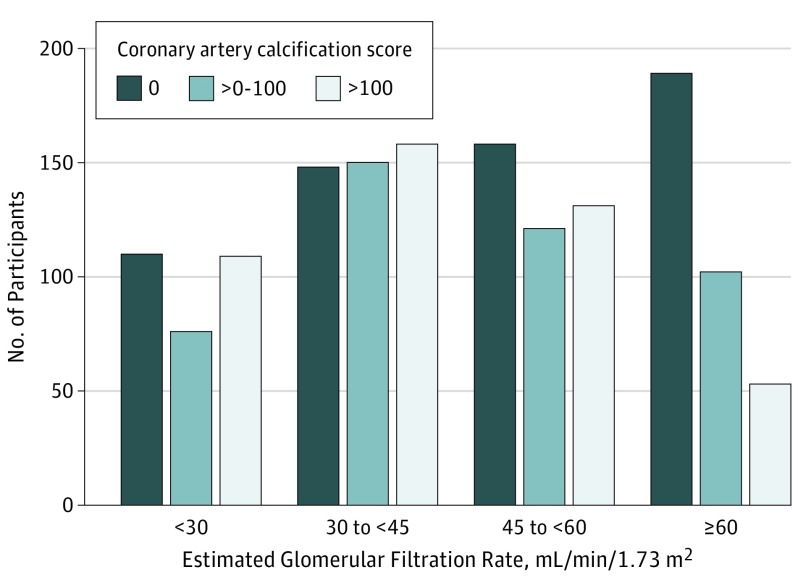
Design, setting, and participants: The prospective Chronic Renal Insufficiency Cohort study recruited adults with an estimated glomerular filtration rate of 20 to 70 mL/min/1.73 m2 from 7 clinical centers in the United States. There were 1541 participants without cardiovascular disease at baseline who had CAC scores.
Exposures: Coronary artery calcification was assessed using electron-beam or multidetector computed tomography.
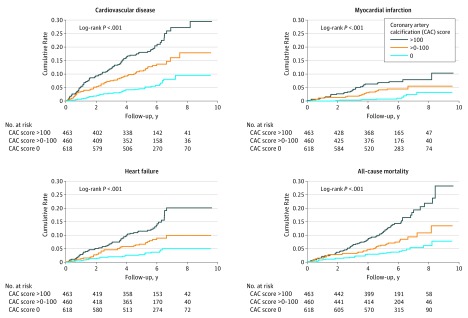
Main outcomes and measures: Incidence of cardiovascular disease (including myocardial infarction, heart failure, and stroke) and all-cause mortality were reported every 6 months and confirmed by medical record adjudication.
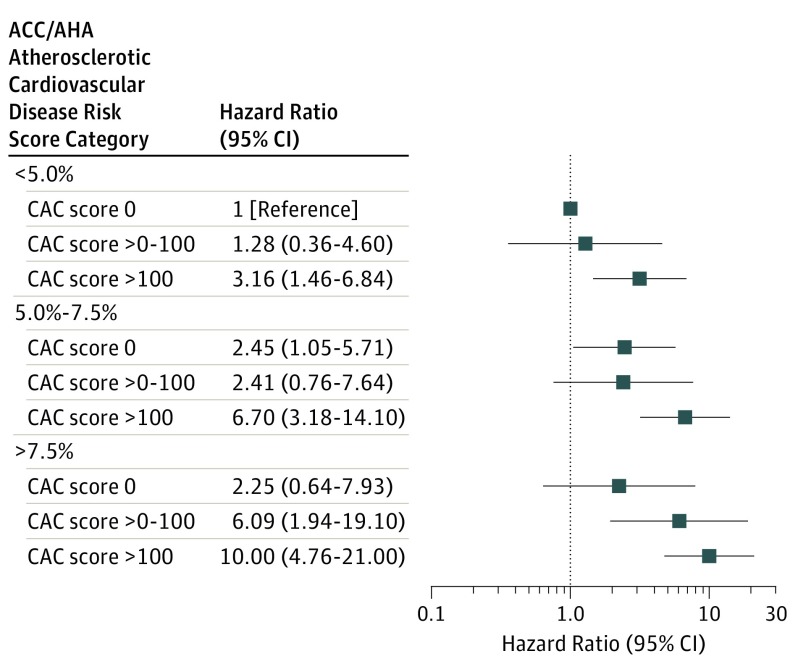
Results: During an average follow-up of 5.9 years in 1541 participants aged 21 to 74 years, there were 188 cardiovascular disease events (60 cases of myocardial infarction, 120 heart failures, and 27 strokes; patients may have had >1 event) and 137 all-cause deaths. In Cox proportional hazards models adjusted for age, sex, race, clinical site, education level, physical activity, total cholesterol level, high-density lipoprotein cholesterol level, systolic blood pressure, use of antihypertensive treatment, current cigarette smoking, diabetes status, body mass index, C-reactive protein level, hemoglobin A1c level, phosphorus level, troponin T level, log N-terminal pro-B-type natriuretic peptide level, fibroblast growth factor 23 level, estimated glomerular filtration rate, and proteinuria, the hazard ratios associated with per 1 SD log of CAC were 1.40 (95% CI, 1.16-1.69; P < .001) for cardiovascular disease, 1.44 (95% CI, 1.02-2.02; P = .04) for myocardial infarction, 1.39 (95% CI, 1.10-1.76; P = .006) for heart failure, and 1.19 (95% CI, 0.94-1.51; P = .15) for all-cause mortality. In addition, inclusion of CAC score led to an increase in the C statistic of 0.02 (95% CI, 0-0.09; P < .001) for predicting cardiovascular disease over use of all the above-mentioned established and novel cardiovascular disease risk factors.
Conclusions and relevance: Coronary artery calcification is independently and significantly related to the risks of cardiovascular disease, myocardial infarction, and heart failure in patients with CKD. In addition, CAC improves risk prediction for cardiovascular disease, myocardial infarction, and heart failure over use of established and novel cardiovascular disease risk factors among patients with CKD; however, the changes in the C statistic are small.
Conflict of interest statement
Figures
Comment in
-
Cardiovascular disease: Coronary artery calcification predicts risk of CVD in patients with CKD.Nat Rev Nephrol. 2017 Jun;13(6):324-326. doi: 10.1038/nrneph.2017.61. Epub 2017 May 8. Nat Rev Nephrol. 2017. PMID: 28480902 No abstract available.
References
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339-352. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305. - PubMed
-
- Matsushita K, van der Velde M, Astor BC, et al. ; Chronic Kidney Disease Prognosis Consortium . Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet. 2010;375(9731):2073-2081. - PMC - PubMed
-
- Hemmelgarn BR, Manns BJ, Lloyd A, et al. ; Alberta Kidney Disease Network . Relation between kidney function, proteinuria, and adverse outcomes. JAMA. 2010;303(5):423-429. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
