

Treatment Response in Enteric Fever in an Era of Increasing Antimicrobial Resistance: An Individual Patient Data Analysis of 2092 Participants Enrolled into 4 Randomized, Controlled Trials in Nepal
- PMID: 28329181
- PMCID: PMC5434338
- DOI: 10.1093/cid/cix185
Treatment Response in Enteric Fever in an Era of Increasing Antimicrobial Resistance: An Individual Patient Data Analysis of 2092 Participants Enrolled into 4 Randomized, Controlled Trials in Nepal
Erratum in
-
Erratum.Clin Infect Dis. 2017 Oct 15;65(8):1431-1433. doi: 10.1093/cid/cix563. Clin Infect Dis. 2017. PMID: 29017252 Free PMC article. No abstract available.
Abstract
Background.: Enteric fever, caused by Salmonella Typhi and Salmonella Paratyphi A, is the leading cause of bacterial febrile disease in South Asia.
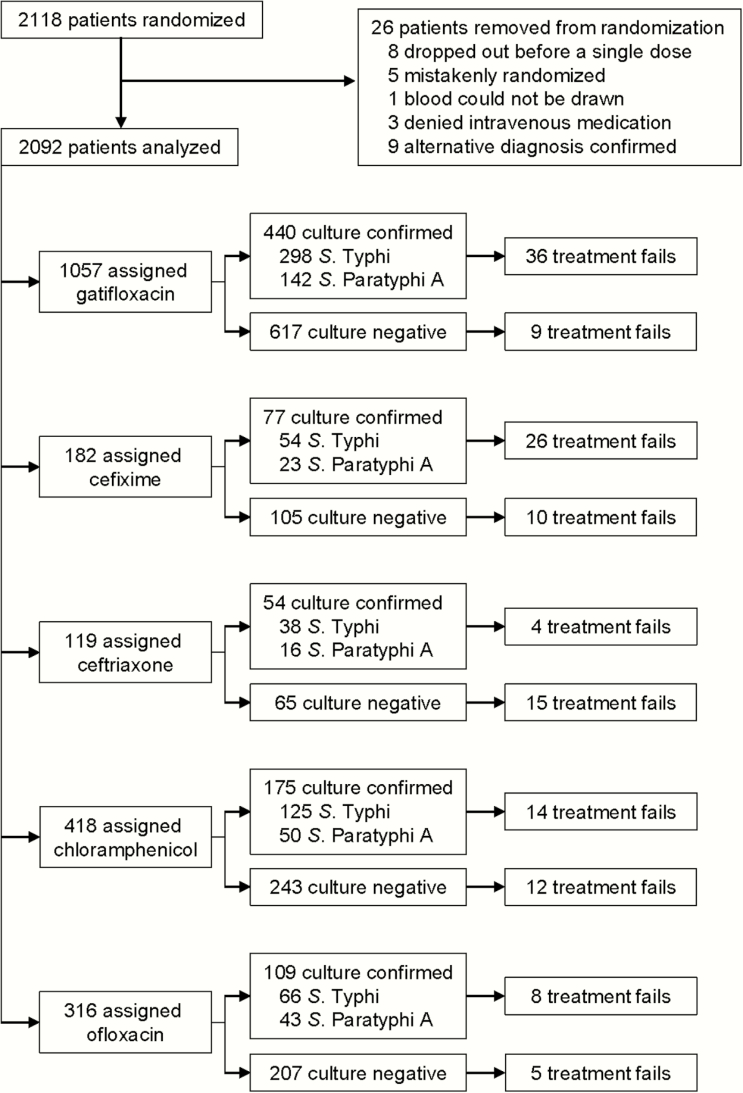
Methods.: Individual data from 2092 patients with enteric fever randomized into 4 trials in Kathmandu, Nepal, were pooled. All trials compared gatifloxacin with 1 of the following comparator drugs: cefixime, chloramphenicol, ofloxacin, or ceftriaxone. Treatment outcomes were evaluated according to antimicrobial if S. Typhi/Paratyphi were isolated from blood. We additionally investigated the impact of changing bacterial antimicrobial susceptibility on outcome.
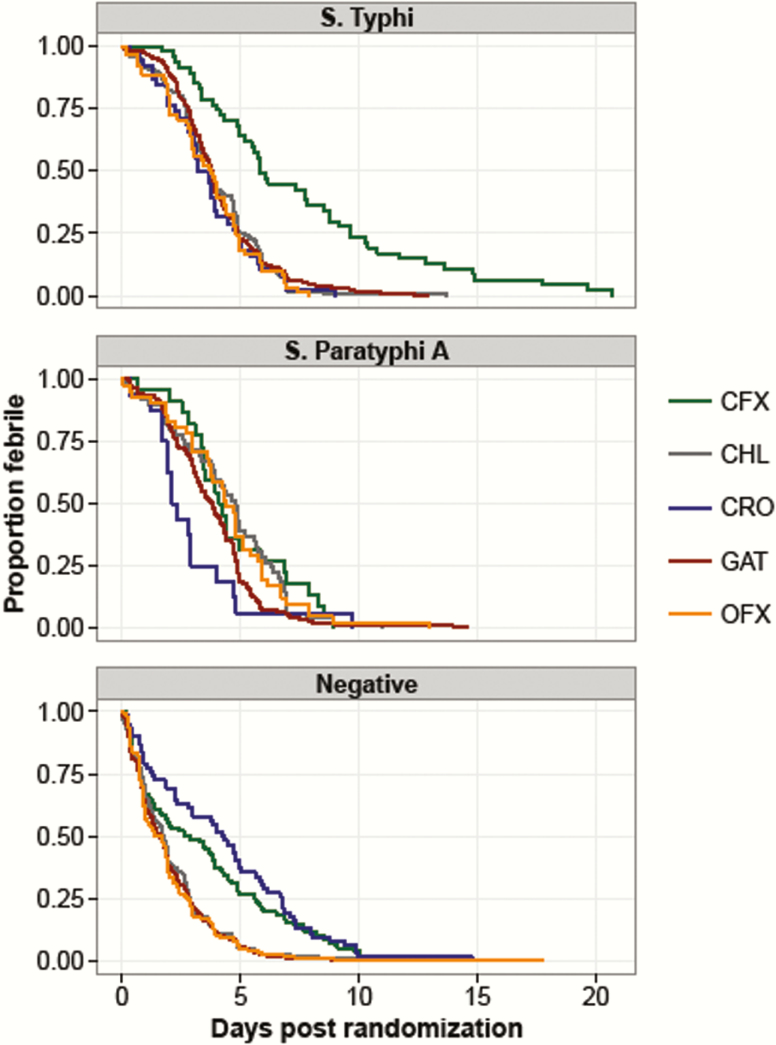
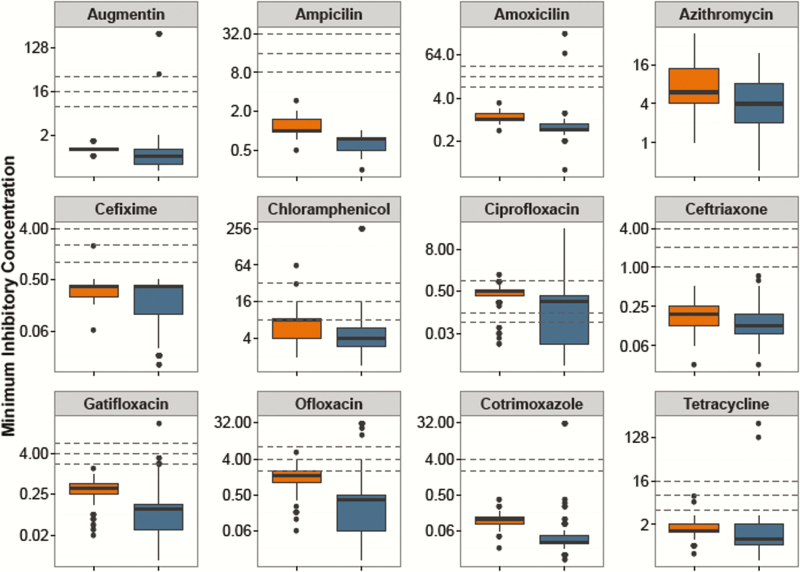
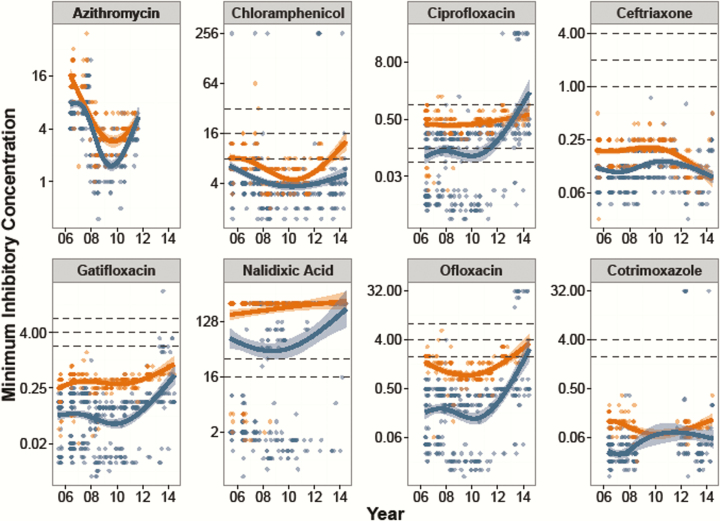
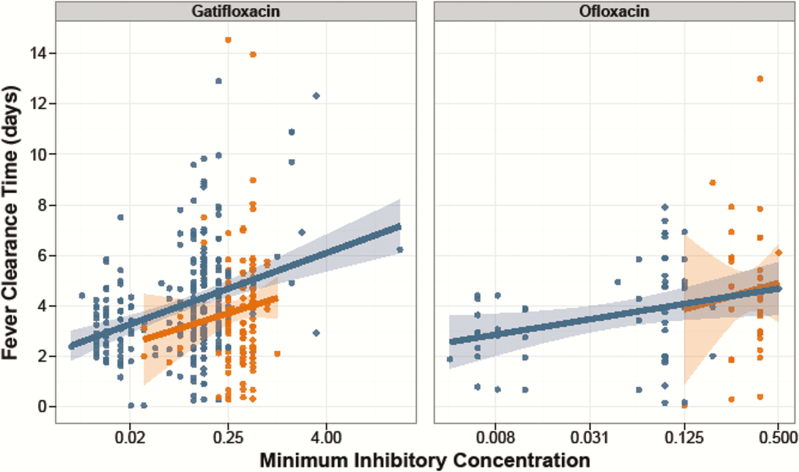
Results.: Overall, 855 (41%) patients had either S. Typhi (n = 581, 28%) or S. Paratyphi A (n = 274, 13%) cultured from blood. There were 139 (6.6%) treatment failures with 1 death. Except for the last trial with ceftriaxone, the fluoroquinolone gatifloxacin was associated with equivalent or better fever clearance times and lower treatment failure rates in comparison to all other antimicrobials. However, we additionally found that the minimum inhibitory concentrations (MICs) against fluoroquinolones have risen significantly since 2005 and were associated with increasing fever clearance times. Notably, all organisms were susceptible to ceftriaxone throughout the study period (2005-2014), and the MICs against azithromycin declined, confirming the utility of these alternative drugs for enteric fever treatment.
Conclusion.: The World Health Organization and local government health ministries in South Asia still recommend fluoroquinolones for enteric fever. This policy should change based on the evidence provided here. Rapid diagnostics are urgently required given the large numbers of suspected enteric fever patients with a negative culture.
Keywords: Nepal; antimicrobial resistance; enteric fever; fluoroquinolone; typhoid.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
