

The Causal Effect of Tracing by Peer Health Workers on Return to Clinic Among Patients Who Were Lost to Follow-up From Antiretroviral Therapy in Eastern Africa: A "Natural Experiment" Arising From Surveillance of Lost Patients
- PMID: 28329184
- PMCID: PMC5848300
- DOI: 10.1093/cid/cix191
The Causal Effect of Tracing by Peer Health Workers on Return to Clinic Among Patients Who Were Lost to Follow-up From Antiretroviral Therapy in Eastern Africa: A "Natural Experiment" Arising From Surveillance of Lost Patients
Erratum in
-
Erratum.Clin Infect Dis. 2017 Oct 15;65(8):1431-1433. doi: 10.1093/cid/cix563. Clin Infect Dis. 2017. PMID: 29017252 Free PMC article. No abstract available.
Abstract
Background.: The effect of tracing human immunodeficiency virus (HIV)-infected patients who are lost to follow-up (LTFU) on reengagement has not been rigorously assessed. We carried out an ex post analysis of a surveillance study in which LTFU patients were randomly selected for tracing to identify the effect of tracing on reengagement.
Methods.: We evaluated HIV-infected adults on antiretroviral therapy who were LTFU (>90 days late for last visit) at 14 clinics in Uganda, Kenya, and Tanzania. A random sample of LTFU patients was selected for tracing by peer health workers. We assessed the effect of selection for tracing using Kaplan-Meier estimates of reengagement among all patients as well as the subset of LTFU patients who were alive, contacted in person by the tracer, and out of care.
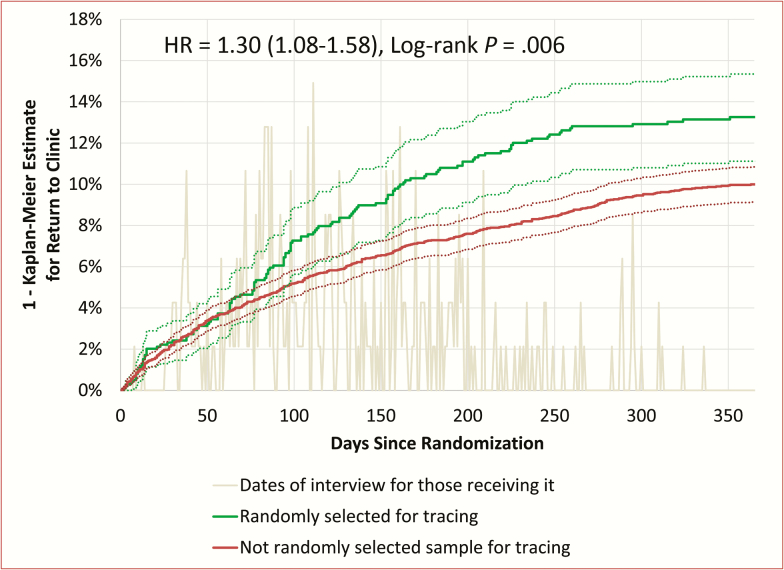
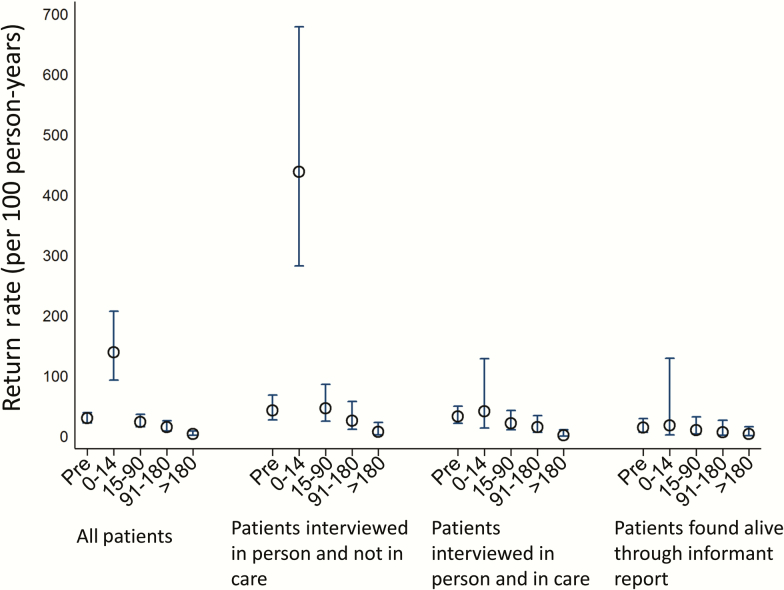
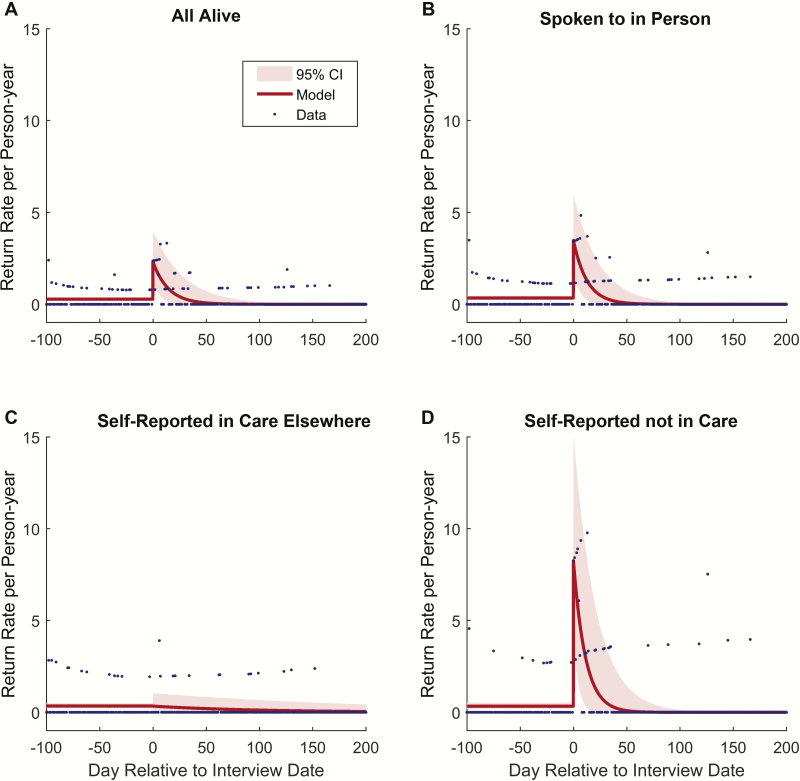
Results.: Of 5781 eligible patients, 991 (17%) were randomly selected for tracing. One year after selection for tracing, 13.3% (95% confidence interval [CI], 11.1%-15.3%) of those selected for tracing returned compared with 10.0% (95% CI, 9.1%-10.8%) of those not randomly selected, an adjusted risk difference of 3.0% (95% CI, .7%-5.3%). Among patients found to be alive, personally contacted, and out of care, tracing increased the absolute probability of return at 1 year by 22% (95% CI, 7.1%-36.2%). The effect of tracing on rate of return to clinic decayed with a half-life of 7.0 days after tracing (95% CI, 2.6 %-12.9%).
Conclusions.: Tracing interventions increase reengagement, but developing methods for targeting LTFU patients most likely to benefit can make this practice more efficient.
Keywords: Africa; antiretroviral therapy; loss to follow-up.; retention.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Patient Tracking as a Tool to Improve Retention in Care: Is the Juice Worth the Squeeze?Clin Infect Dis. 2017 Jun 1;64(11):1555-1556. doi: 10.1093/cid/cix196. Clin Infect Dis. 2017. PMID: 28329039 No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
