

Systematic Review, Meta-analysis, and Cost-effectiveness of Treatment of Latent Tuberculosis to Reduce Progression to Multidrug-Resistant Tuberculosis
- PMID: 28329197
- PMCID: PMC5543758
- DOI: 10.1093/cid/cix208
Systematic Review, Meta-analysis, and Cost-effectiveness of Treatment of Latent Tuberculosis to Reduce Progression to Multidrug-Resistant Tuberculosis
Erratum in
-
Erratum.Clin Infect Dis. 2017 Oct 15;65(8):1433-1434. doi: 10.1093/cid/cix576. Clin Infect Dis. 2017. PMID: 29017257 No abstract available.
Abstract
Background.: Evidence-based recommendations for treating persons having presumed latent tuberculosis (LTBI) after contact to infectious multidrug-resistant (MDR) tuberculosis (TB) are lacking because published data consist of small observational studies. Tuberculosis incidence in persons treated for latent MDR -TB infection is unknown.
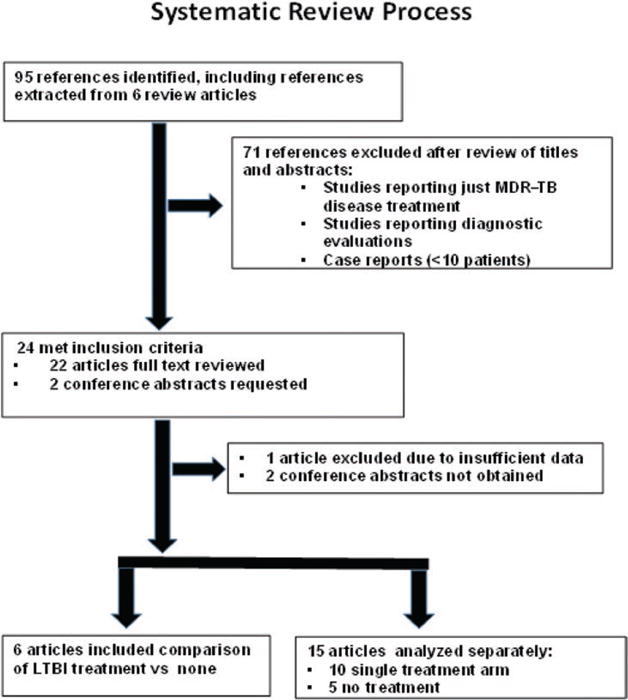
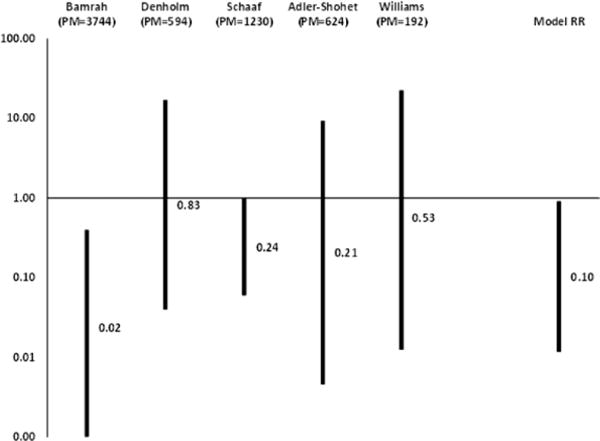
Methods.: We conducted a systematic review of studies published 1 January 1994-31 December 2014 to analyze TB incidence, treatment completion and discontinuation, and cost-effectiveness. We considered contacts with LTBI effectively treated if they were on ≥1 medication to which their MDR-TB strain was likely susceptible. We selected studies that compared treatment vs nontreatment outcomes and performed a meta-analysis to estimate the relative risk of TB incidence and its 95% confidence interval.
Results.: We abstracted data from 21 articles that met inclusion criteria. Six articles presented outcomes for contacts who were treated compared with those not treated for MDR-LTBI; 10 presented outcomes only for treated contacts, and 5 presented outcomes only for untreated contacts. The estimated MDR-TB incidence reduction was 90% (9%-99%) using data from 5 comparison studies. We also found high treatment discontinuation rates due to adverse effects in persons taking pyrazinamide-containing regimens. Cost-effectiveness was greatest using a fluoroquinolone/ethambutol combination regimen.
Conclusions.: Few studies met inclusion criteria, therefore results should be cautiously interpreted. We found a reduced risk of TB incidence with treatment for MDR-LTBI, suggesting effectiveness in prevention of progression to MDR-TB, and confirmed cost-effectiveness. However, we found that pyrazinamide-containing MDR-LTBI regimens often resulted in treatment discontinuation due to adverse effects.
Keywords: contacts; cost.; multidrug-resistant; treatment; tuberculosis.
Published by Oxford University Press for the Infectious Diseases Society of America 2017. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Conflict of interest statement
Figures
References
-
- Research Excellence to Stop TB Resistance. Drug-resistant tuberculosis clinical trials progress report. Available at: http://www.resisttb.org/?page_id=1602. Accessed 9 February 2017.
-
- Centers for Disease Control and Prevention. Management of persons exposed to multidrug-resistant tuberculosis. MMWR Recomm Rep. 1992;41:61–71. - PubMed
-
- Curry International Tuberculosis Center and California Department of Public Health. Drug-resistant tuberculosis: a survival guide for clinicians. (3rd) :284–289. Available at: http://www.currytbcenter.ucsf.edu/products/cover-pages/drug-resistant-tu.... Accessed June 2016.
-
- Seddon JA, Fred D, Amanullah F, et al. Policy Brief No 1. Dubai, UAE: Harvard Medical School Center for Global Health Delivery-Dubai; 2015. Post-exposure management of multidrug-resistant tuberculosis contacts: evidence-based recommendations.
-
- Cochrane Handbook for Systematic Reviews of Interventions. Available at: http://training.cochrane.org/handbook. Accessed October 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
