

Practice Patterns and Outcomes Associated With Procalcitonin Use in Critically Ill Patients With Sepsis
- PMID: 28329238
- PMCID: PMC5434362
- DOI: 10.1093/cid/cix179
Practice Patterns and Outcomes Associated With Procalcitonin Use in Critically Ill Patients With Sepsis
Erratum in
-
Erratum.Clin Infect Dis. 2017 Oct 15;65(8):1431-1433. doi: 10.1093/cid/cix563. Clin Infect Dis. 2017. PMID: 29017252 Free PMC article. No abstract available.
Abstract
Background.: Randomized trials support use of procalcitonin (PCT)-based algorithms to decrease duration of antibiotics for critically ill patients with sepsis. However, current use of PCT and associated outcomes in real-world clinical settings is unclear. We sought to determine PCT use in critically ill patients with sepsis in the United States and to examine associations between PCT use and clinical outcomes.
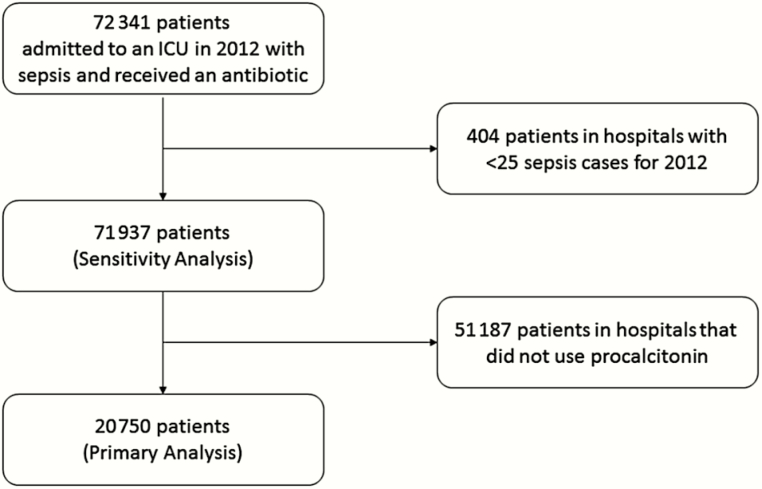
Methods.: This was a retrospective cohort study of approximately 20% of patients with sepsis hospitalized in US intensive care units. Hierarchical regression models were used to determine associations of PCT use with outcomes (antibiotic-days, incidence of Clostridium difficile infection, and in-hospital mortality). Sensitivity analyses were conducted to assess robustness of findings to different methods used to address unmeasured confounding (eg, instrumental variable, difference-in-differences analyses).
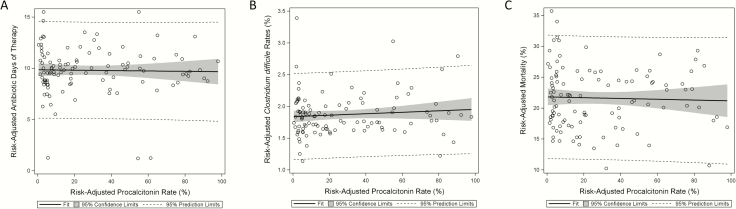
Results.: Among 20750 critically ill patients with sepsis in 107 hospitals with PCT available, 3769 (18%) patients had PCT levels checked; 1119 (29.7%) had serial PCT measurements. PCT use was associated with increased antibiotic-days (adjusted relative risk, 1.1; 95% confidence interval [CI], 1.15-1.18) and incidence of C. difficile (adjusted odds ratio, 1.42; 95% CI, 1.09-1.85) without a change in mortality (adjusted hazard ratio, 1.05; 95% CI, 0.93-1.19). Analysis of PCT use by instrumental variable and difference-in-difference analyses showed similar lack of antibiotic or outcome improvements associated with PCT use.
Conclusions.: PCT use was not associated with improved antibiotic use or other clinical outcomes in real-world settings. Programs to improve implementation of PCT-based strategies are warranted prior to widespread adoption.
Keywords: Clostridium difficile.; antibacterial agents/administration and dosage; critical care; outcome assessment.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com
Figures
References
-
- Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014; 312:90–2. - PubMed
-
- Van Boeckel TP, Gandra S, Ashok A, et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis 2014; 14: 742–50. - PubMed
-
- Hecker MT, Aron DC, Patel NP, Lehmann MK, Donskey CJ. Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch Intern Med 2003; 163:972–8. - PubMed
-
- Christ-Crain M, Jaccard-Stolz D, Bingisser R, et al. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: cluster-randomised, single-blinded intervention trial. Lancet 2004; 363:600–7. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
