

Utilization and in-hospital complications of cardiac resynchronization therapy: trends in the United States from 2003 to 2013
- PMID: 28329322
- PMCID: PMC5837705
- DOI: 10.1093/eurheartj/ehx100
Utilization and in-hospital complications of cardiac resynchronization therapy: trends in the United States from 2003 to 2013
Abstract
Aims: Cardiac resynchronization therapy (CRT) device implantation has been shown to reduce morbidity and mortality in selected patients with heart failure. We sought to investigate the utilization and in-hospital complications of cardiac resynchronization therapy defibrillator (CRT-D) and pacemaker (CRT-P) implantations in the United States from 2003 to 2013.
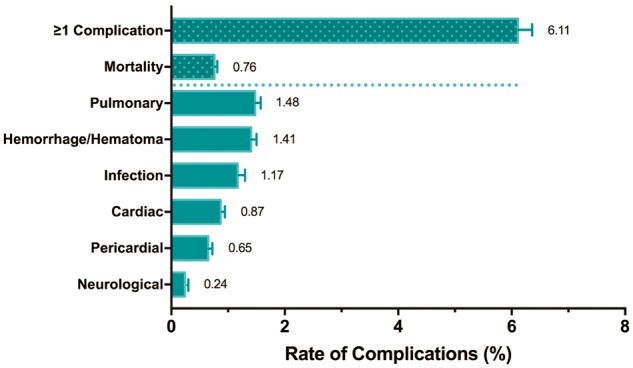
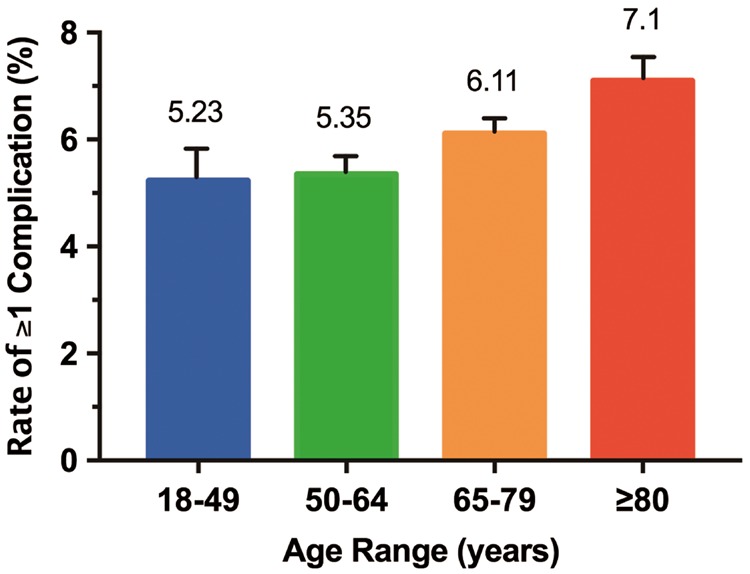
Methods and results: Patients receiving CRT-D or CRT-P were identified in the National Inpatient Sample database (NIS), using the International Classification of Diseases-Ninth Revision-Clinical Modification procedure codes. Annual implantation rates, patient demographics, co-morbidities, in-hospital complications, and length of stay were analysed. From 2003 to 2013, an estimated total of 439 010 (95% CI: 406 723-471 296) inpatient CRT implantations were performed in the U.S. The median age of patients was 72 and 71% were male. Overall, 6.1% had at least one complication. During the study period, comorbidity index and overall complication rate increased (P = 0.002 and P = 0.01, respectively). Mortality and length of stay showed no significant trend. Predictors of complications included: age 65 and older, female sex (OR: 1.19; 95% CI: 1.12-1.27), Deyo-Charlson Comorbidity Index, and elective admission (OR: 0.61; 95% CI: 0.57-0.66).
Conclusion: From 2003 to 2013, the severity of comorbid conditions increased and a rising trend was observed in the rate of periprocedural complications among patients undergoing CRT in the United States. In-hospital mortality and length of stay showed no uniform trend.
Keywords: Cardiac resynchronization therapy; Complication; Defibrillator; Pacemaker.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2017. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Cardiac resynchronization therapy in the real world: need to focus on implant rates, patient selection, co-morbidities, type of devices, and complications.Eur Heart J. 2017 Jul 14;38(27):2129-2131. doi: 10.1093/eurheartj/ehx137. Eur Heart J. 2017. PMID: 28430905 No abstract available.
References
-
- Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, DeVries DW, Feldman AM.. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med 2004;350:2140–2150. - PubMed
-
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL, Ellestad M, Trupp RJ, Underwood J, Pickering F, Truex C, McAtee P, Messenger J.. Cardiac resynchronization in chronic heart failure. N Engl J Med 2002;346:1845–1853. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NAMIII, Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D, Zareba W.. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med 2009;361:1329–1338. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
