

Costs and Consequences of Early Hospital Discharge After Major Inpatient Surgery in Older Adults
- PMID: 28329352
- PMCID: PMC5478875
- DOI: 10.1001/jamasurg.2017.0123
Costs and Consequences of Early Hospital Discharge After Major Inpatient Surgery in Older Adults
Abstract
Importance: As prospective payment transitions to bundled reimbursement, many US hospitals are implementing protocols to shorten hospitalization after major surgery. These efforts could have unintended consequences and increase overall surgical episode spending if they induce more frequent postdischarge care use or readmissions.
Objective: To evaluate the association between early postoperative discharge practices and overall surgical episode spending and expenditures for postdischarge care use and readmissions.
Design, setting, and participants: This investigation was a cross-sectional cohort study of Medicare beneficiaries undergoing colectomy (189 229 patients at 1876 hospitals), coronary artery bypass grafting (CABG) (218 940 patients at 1056 hospitals), or total hip replacement (THR) (231 774 patients at 1831 hospitals) between January 1, 2009, and June 30, 2012. The dates of the analysis were September 1, 2015, to May 31, 2016. Associations between surgical episode payments and hospitals' length of stay (LOS) mode were evaluated among a risk and postoperative complication-matched cohort of patients without major postoperative complications. To further control for potential differences between hospitals, a within-hospital comparison was also performed evaluating the change in hospitals' mean surgical episode payments according to their change in LOS mode during the study period.
Exposure: Undergoing surgery in a hospital with short vs long postoperative hospitalization practices, characterized according to LOS mode, a measure least sensitive to postoperative outliers.
Main outcomes and measures: Risk-adjusted, price-standardized, 90-day overall surgical episode payments and their components, including index, outlier, readmission, physician services, and postdischarge care.
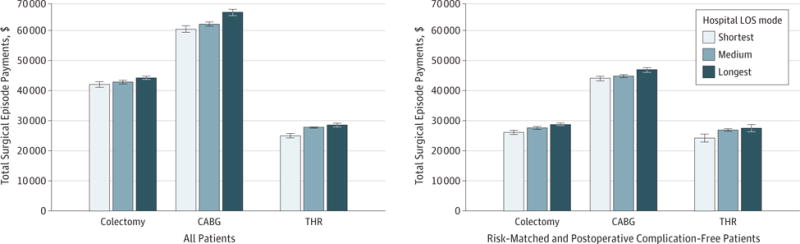
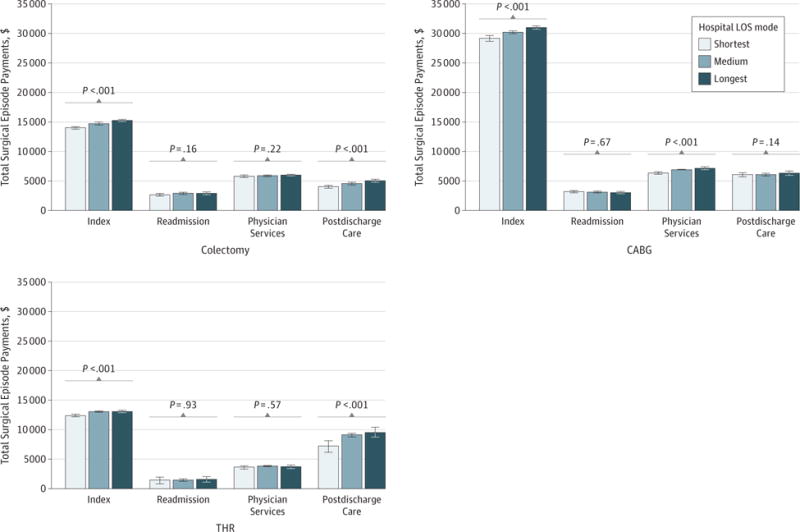
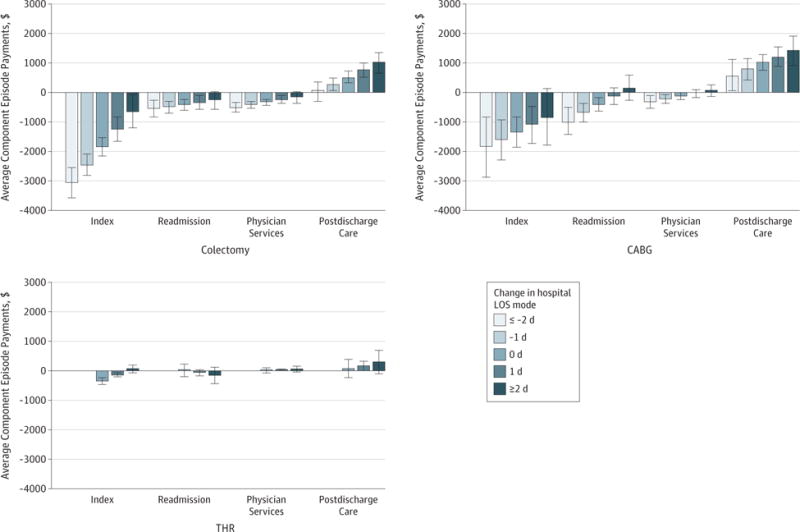
Results: A total of 639 943 Medicare beneficiaries were included in the study. Total surgical episode payments for risk and postoperative complication-matched patients were significantly lower among hospitals with lowest vs highest LOS mode ($26 482 vs $29 250 for colectomy, $44 777 vs $47 675 for CABG, and $24 553 vs $27 927 for THR; P < .001 for all). Shortest LOS hospitals did not exhibit a compensatory increase in payments for postdischarge care use ($4011 vs $5083 for colectomy, P < .001; $6015 vs $6355 for CABG, P = .14; and $7132 vs $9552 for THR, P < .001) or readmissions ($2606 vs $2887 for colectomy, P = .16; $3175 vs $3064 for CABG, P = .67; and $1373 vs $1514 for THR, P = .93). Hospitals that exhibited the greatest decreases in LOS mode had the highest reductions in surgical episode payments during the study period.
Conclusions and relevance: Early routine postoperative discharge after major inpatient surgery is associated with lower total surgical episode payments. There is no evidence that savings from shorter postsurgical hospitalization are offset by higher postdischarge care spending. Therefore, accelerated postoperative care protocols appear well aligned with the goals of bundled payment initiatives for surgical episodes.
Conflict of interest statement
Figures
References
-
- Cowper PA, DeLong ER, Hannan EL, et al. Trends in postoperative length of stay after bypass surgery. Am Heart J. 2006;152(6):1194–1200. - PubMed
-
- Cowper PA, DeLong ER, Hannan EL, et al. Is early too early? effect of shorter stays after bypass surgery. Ann Thorac Surg. 2007;83(1):100–10. - PubMed
-
- Wolford ML, Palso K, Bercovitz A. Hospitalization for total hip replacement among inpatients aged 45 and over: United States, 2000–2010. NCHS Data Brief. 2015;(186):1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
