

Clinical Significance of Human Coronavirus in Bronchoalveolar Lavage Samples From Hematopoietic Cell Transplant Recipients and Patients With Hematologic Malignancies
- PMID: 28329354
- PMCID: PMC5434339
- DOI: 10.1093/cid/cix160
Clinical Significance of Human Coronavirus in Bronchoalveolar Lavage Samples From Hematopoietic Cell Transplant Recipients and Patients With Hematologic Malignancies
Erratum in
-
Erratum.Clin Infect Dis. 2017 Oct 15;65(8):1431-1433. doi: 10.1093/cid/cix563. Clin Infect Dis. 2017. PMID: 29017252 Free PMC article. No abstract available.
Abstract
Background.: The possible role of human coronavirus (HCoV) in lower respiratory tract disease (LRTD) in hematopoietic cell transplant (HCT) recipients and patients with hematologic malignancies (HM) has not been well studied.
Methods.: We conducted a retrospective review of HCT/HM patients with HCoV detected in bronchoalveolar lavage (BAL). HCoV strains were identified in BAL samples using strain-specific polymerase chain reaction. Mortality rates were compared among HCT recipients with LRTD caused by HCoV, respiratory syncytial virus (RSV), influenza virus, or parainfluenza virus (PIV) by multivariable Cox regression analysis.
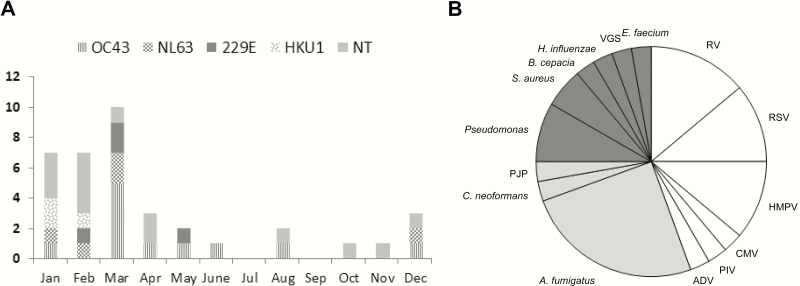
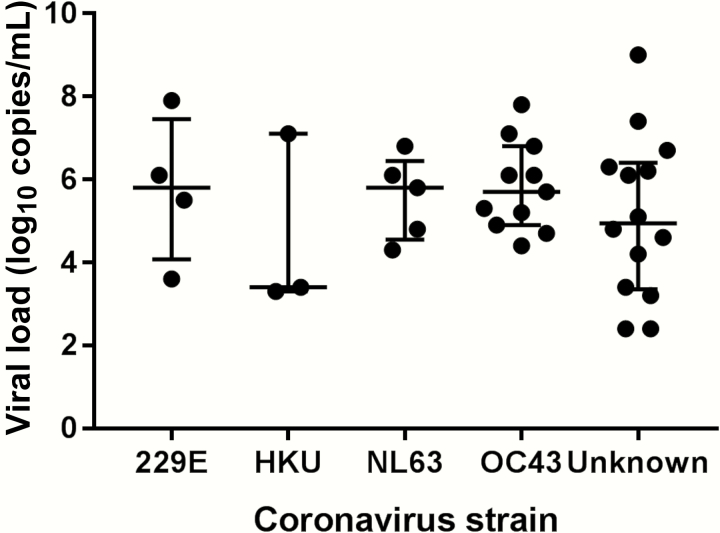
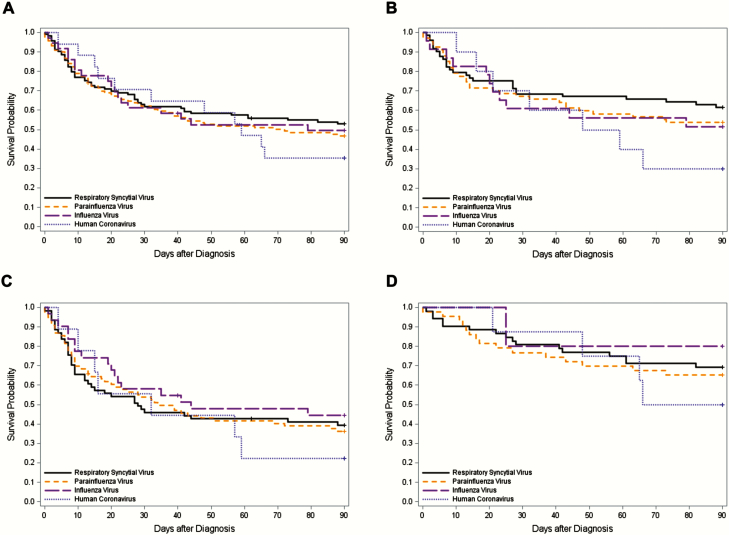
Results.: We identified 35 patients (37 episodes) with HCoV LRTD. Among 23 available BAL samples, 48% were strain OC43, 22% were NL63, 17% were 229E, and 13% were HKU1. Overall, 21 patients (60%) required oxygen therapy at diagnosis and 19 (54%) died within 90 days of diagnosis. Respiratory copathogens were detected in 21 episodes (57%), including viruses (n = 12), fungi (n = 10), and bacteria (n = 8). Mortality rates were not different between patients with and without copathogens (P = .65). In multivariable models, mortality associated with HCoV LRTD was similar to that seen with RSV, influenza, and PIV LRTD in HCT recipients (adjusted hazard ratio, 1.34 [95% confidence interval, .66-2.71], P = .41 vs RSV, adjusted for cell source, cytopenia, copathogens, oxygen use, and steroid use).
Conclusions.: HCoV LRTD in patients with HCT or HM is associated with high rates of oxygen use and mortality. Mortality associated with HCoV LRTD in HCT recipients appears to be similar to that seen with RSV, influenza virus, and PIV.
Keywords: bronchoalveolar lavage; hematologic malignancy.; hematopoietic cell transplant; human coronavirus; lower respiratory tract disease.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com
Figures
References
-
- Lo MS, Lee GM, Gunawardane N, Burchett SK, Lachenauer CS, Lehmann LE. The impact of RSV, adenovirus, influenza, and parainfluenza infection in pediatric patients receiving stem cell transplant, solid organ transplant, or cancer chemotherapy. Pediatr Transplant 2013; 17:133–43. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
