

Systemic Immunomodulating Therapies for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis
- PMID: 28329382
- PMCID: PMC5817620
- DOI: 10.1001/jamadermatol.2016.5668
Systemic Immunomodulating Therapies for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis
Abstract
Importance: Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN) are rare but severe adverse reactions with high mortality. There is no evidence-based treatment, but various systemic immunomodulating therapies are used.
Objectives: To provide an overview on possible immunomodulating treatments for SJS/TEN and estimate their effects on mortality compared with supportive care.
Data sources: A literature search was performed in December 2012 for articles published in MEDLINE, MEDLINE Daily, MEDLINE Inprocess, Web of Science, EMBASE, Scopus, and the Cochrane Library (Central) from January 1990 through December 2012, and updated in December 2015, in the English, French, Spanish, and German languages looking for treatment proposals for SJS/TEN. Other sources were screened manually.
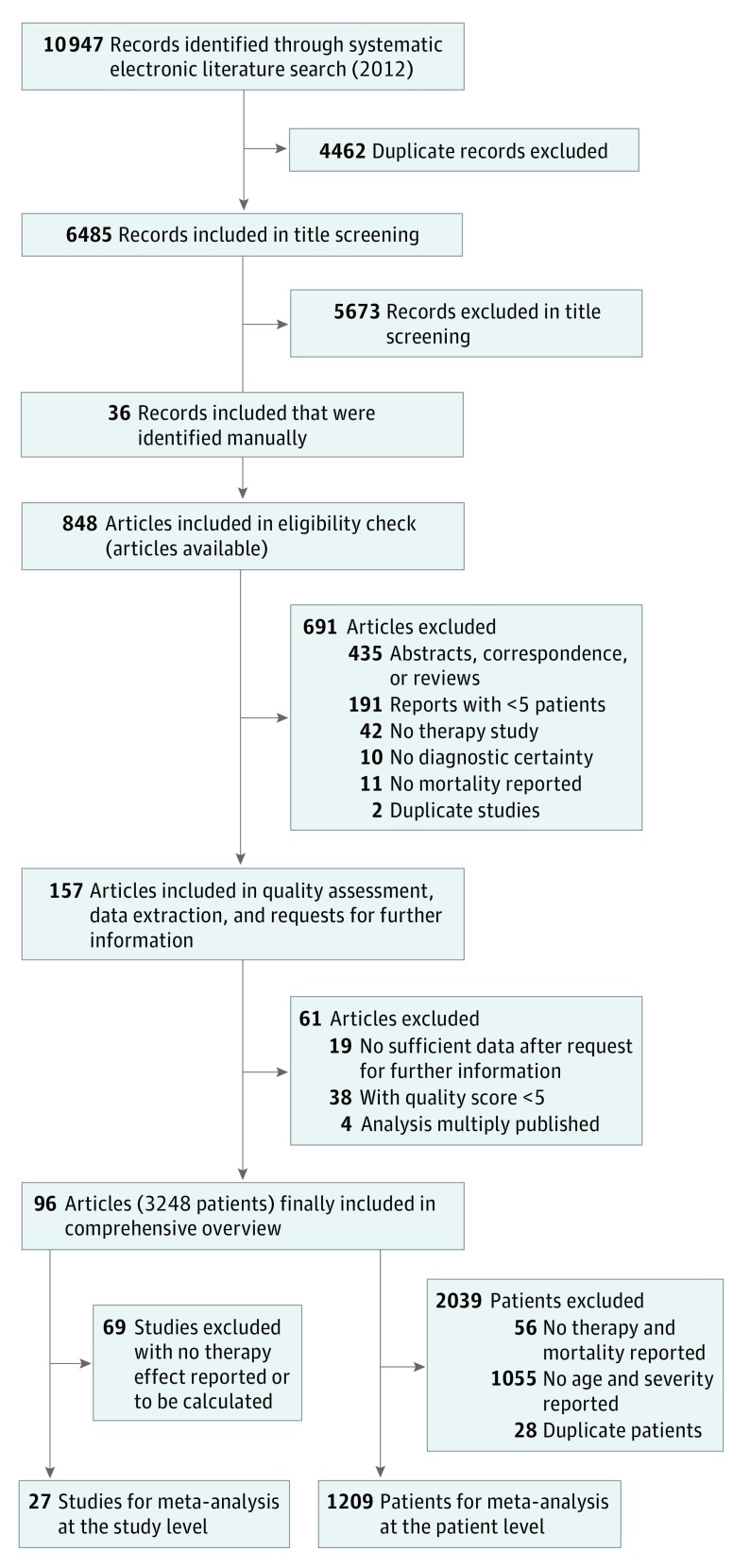
Study selection: Initially, 157 randomized and nonrandomized studies on therapies (systemic immunomodulating therapies or supportive care) for SJS/TEN were selected.
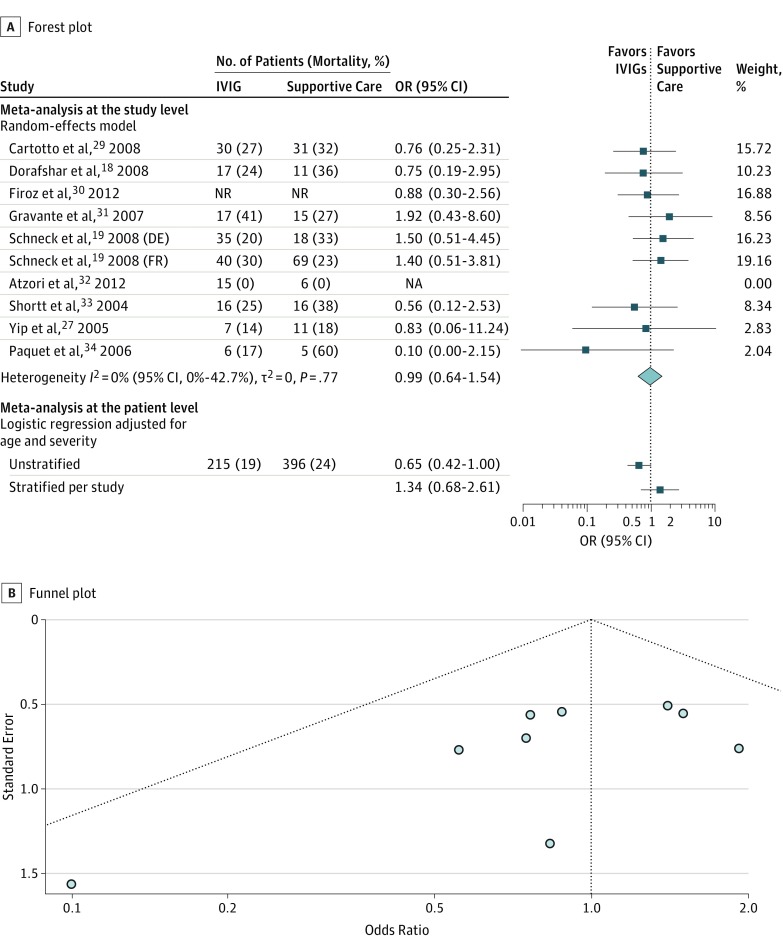
Data extraction and synthesis: Relevant data were extracted from articles. Authors were contacted for further information. Finally, 96 studies with sufficient information regarding eligibility and adequate quality scores were considered in the data synthesis. All steps were performed independently by 2 investigators. Meta-analyses on aggregated study data (random-effects model) and individual patient data (IPD) (logistic regression adjusted for confounders) were performed to assess therapeutic efficacy. In the analysis of IPD, 2 regression models, stratified and unstratified by study, were fitted.
Main outcomes and measures: Therapy effects on mortality were expressed in terms of odds ratios (ORs) with 95% CIs.
Results: Overall, 96 studies (3248 patients) were included. Applied therapies were supportive care or systemic immunomodulating therapies, including glucocorticosteroids, intravenous immunoglobulins, cyclosporine, plasmapheresis, thalidomide, cyclophosphamide, hemoperfusion, tumor necrosis factor inhibitors, and granulocyte colony-stimulating factors. Glucocorticosteroids were associated with a survival benefit for patients in all 3 analyses but were statistically significant in only one (aggregated data: OR, 0.5; 95%% CI, 0.3-1.01; IPD, unstratified: OR, 0.7; 95% CI, 0.5-0.97; IPD, stratified: OR, 0.8; 95% CI, 0.4-1.3). Despite the low patient size, cyclosporine was associated with a promising significant result in the only feasible analysis of IPD (unstratified model) (OR, 0.1; 95% CI, 0.0-0.4). No beneficial findings were observed for other therapies, including intravenous immunoglobulins.
Conclusions and relevance: Although all analyses, including the unstratified model, had limitations, glucocorticosteroids and cyclosporine were the most promising systemic immunomodulating therapies for SJS/TEN. Further evaluation in prospective studies is required. However, this work provides a comprehensive overview on proposed systemic immunomodulating treatments for SJS/TEN, which is of great relevance for treating physicians.
Conflict of interest statement
Figures


References
-
- Paulmann M, Mockenhaupt M. Severe drug-induced skin reactions: clinical features, diagnosis, etiology, and therapy. J Dtsch Dermatol Ges. 2015;13(7):625-645. - PubMed
-
- Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens-Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129(1):92-96. - PubMed
-
- Chung WH, Hung SI, Yang JY, et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Med. 2008;14(12):1343-1350. - PubMed
-
- Heng YK, Lee HY, Roujeau JC. Epidermal necrolysis: 60 years of errors and advances. Br J Dermatol. 2015;173(5):1250-1254. - PubMed
-
- Sekula P, Dunant A, Mockenhaupt M, et al. ; RegiSCAR study group . Comprehensive survival analysis of a cohort of patients with Stevens-Johnson syndrome and toxic epidermal necrolysis. J Invest Dermatol. 2013;133(5):1197-1204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
