

Sepsis recognition in the emergency department - impact on quality of care and outcome?
- PMID: 28330460
- PMCID: PMC5363055
- DOI: 10.1186/s12873-017-0122-9
Sepsis recognition in the emergency department - impact on quality of care and outcome?
Abstract
Background: Appropriate and timely recognition of sepsis is a prerequisite for starting goal-directed therapy bundles. We analyzed the appropriateness of sepsis recognition and documentation with regard to adequacy of therapy and outcome in an internal medicine emergency department (ED).
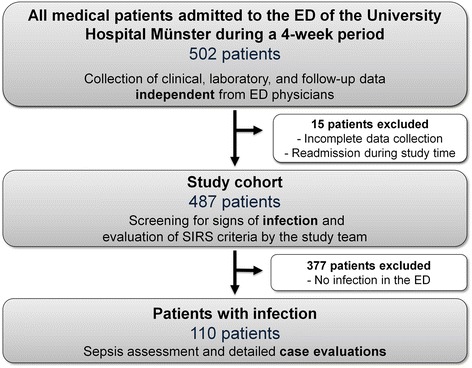
Methods: This study included 487 consecutive patients ≥18 years of age who presented to a university hospital ED during a 4-week period. Clinical, laboratory, and follow-up data were acquired independently from documentation by ED physicians. The study team independently rated quality of sepsis classification (American College of Chest Physicians/Society of Critical Care Medicine definitions), diagnostic workup, and guideline-adherent therapy in the ED.
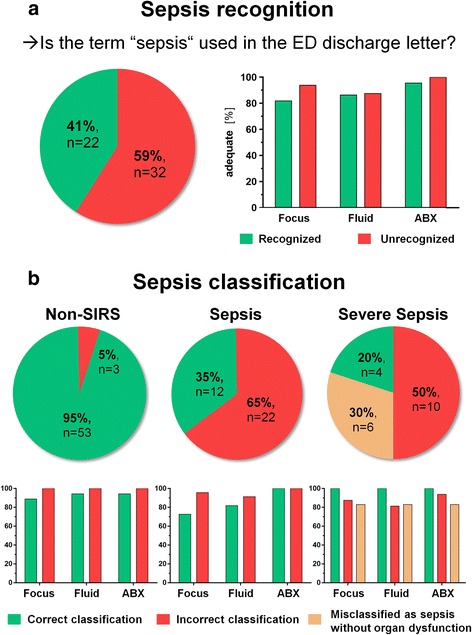
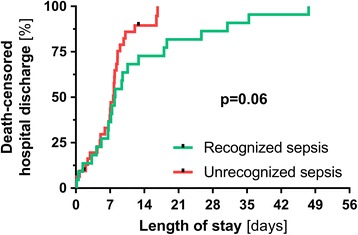
Results: Of 487 included patients, 110 presented because of infection. Of those, 54 patients matched sepsis criteria, including 20 with organ damage and thus severe sepsis, as rated by the study team. Sepsis was not recognized in 32 of these 54 cases (59%). Multivariate binary logistic regression analysis revealed that higher systolic blood pressure (p <0.05), the ability to stand (p <0.01) and a low number of documented vital signs in the ED discharge letter (p < 0.05) were independent predictors of missed sepsis. Surprisingly, adequate detection of the septic focus (81 vs. 93%, p = 0.17), appropriate fluid administration (86 vs. 87%, p = 0.39), and guideline-adherent antibiotic regimen (95 vs. 100%, p = 0.42) did not differ between cases of recognized and unrecognized sepsis, respectively. Non-recognition affected neither death-censored length of hospital stay (median 7.63 d vs. 7.13 d, p = 0.42) nor a combined endpoint of death or ICU admission to (9 vs. 12%, p = 0.55).
Conclusions: Non-recognition of sepsis in ED patients with serious infections who formally meet organizational sepsis definitions seems to have no deleterious impact on initial therapy adequacy.
Keywords: Emergency department; Infection; Quality of care; Sepsis; Sepsis recognition; Severe sepsis.
Figures
References
-
- Alberti C, Brun-Buisson C, Burchardi H, Martin C, Goodman S, Artigas A, Sicignano A, Palazzo M, Moreno R, Boulme R, et al. Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Med. 2002;28(2):108–121. doi: 10.1007/s00134-001-1143-z. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
