Limb flexion-induced twist and associated intramural stresses in the human femoropopliteal artery
- PMID: 28330991
- PMCID: PMC5378143
- DOI: 10.1098/rsif.2017.0025
Limb flexion-induced twist and associated intramural stresses in the human femoropopliteal artery
Abstract
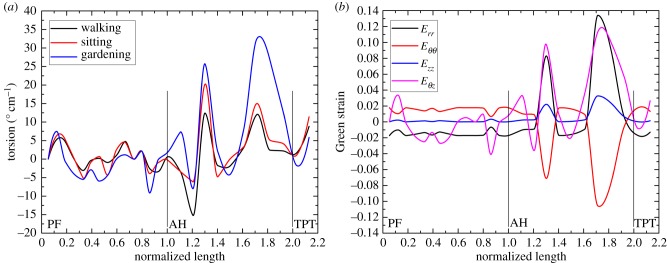
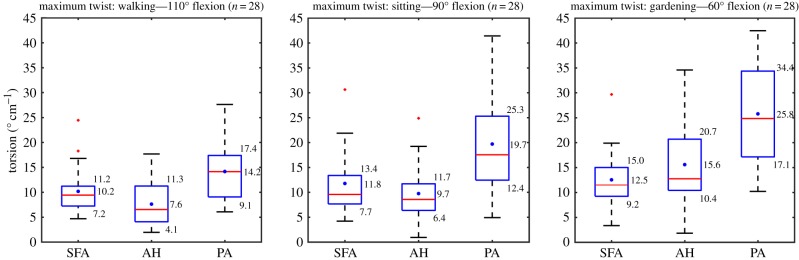
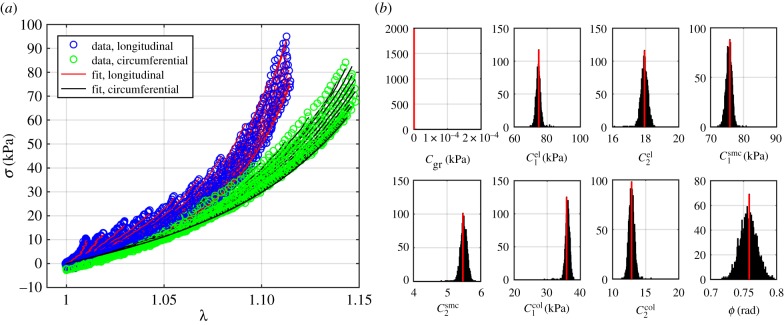
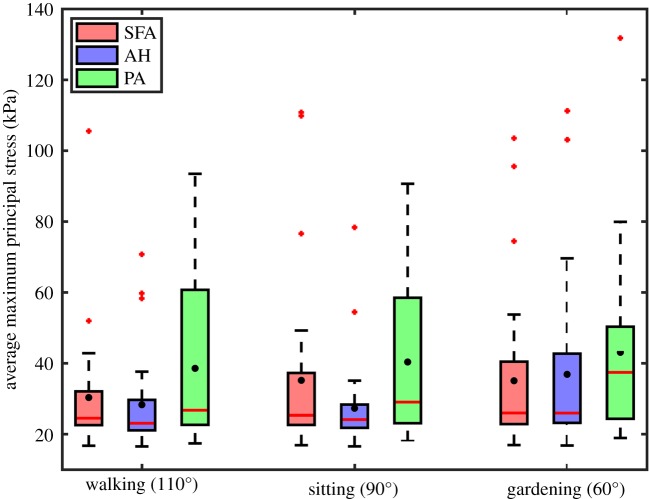
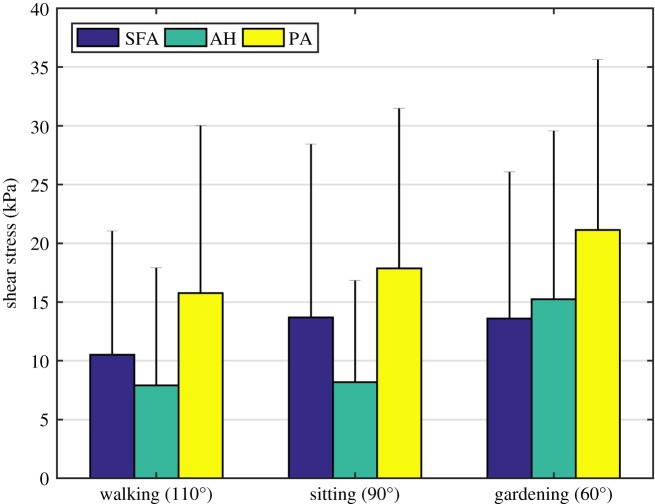
High failure rates of femoropopliteal artery (FPA) interventions are often attributed to severe mechanical deformations that occur with limb movement. Torsion of the FPA likely plays a significant role, but is poorly characterized and the associated intramural stresses are currently unknown. FPA torsion in the walking, sitting and gardening postures was characterized in n = 28 in situ FPAs using intra-arterial markers. Principal mechanical stresses and strains were quantified in the superficial femoral artery (SFA), adductor hiatus segment (AH) and the popliteal artery (PA) using analytical modelling. The FPA experienced significant torsion during limb flexion that was most severe in the gardening posture. The associated mechanical stresses were non-uniformly distributed along the length of the artery, increasing distally and achieving maximum values in the PA. Maximum twist in the SFA ranged 10-13° cm-1, at the AH 8-16° cm-1, and in the PA 14-26° cm-1 in the walking, sitting and gardening postures. Maximum principal stresses were 30-35 kPa in the SFA, 27-37 kPa at the AH and 39-43 kPa in the PA. Understanding torsional deformations and intramural stresses in the FPA can assist with device selection for peripheral arterial disease interventions and may help guide the development of devices with improved characteristics.
Keywords: femoropopliteal artery; intra-arterial markers; mechanical stress; peripheral artery disease; torsion.
© 2017 The Author(s).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources