

Chronological changes in lung cancer surgery in a single Japanese institution
- PMID: 28331339
- PMCID: PMC5348071
- DOI: 10.2147/OTT.S120556
Chronological changes in lung cancer surgery in a single Japanese institution
Abstract
Background: The aim of this study was to evaluate the chronological changes in epidemiological factors and surgical outcomes in patients with lung cancer who underwent surgery in a single Japanese institution.
Patients and methods: A clinicopathological database of patients with lung cancer who underwent surgery with curative intent from January 1974 to December 2014 was reviewed. The chronological changes in various factors, including patient's age, sex, histological type, tumor size, pathological stage (p-stage), surgical method, operative time, intraoperative blood loss, 30-day mortality, and postoperative overall survival (OS), were evaluated.
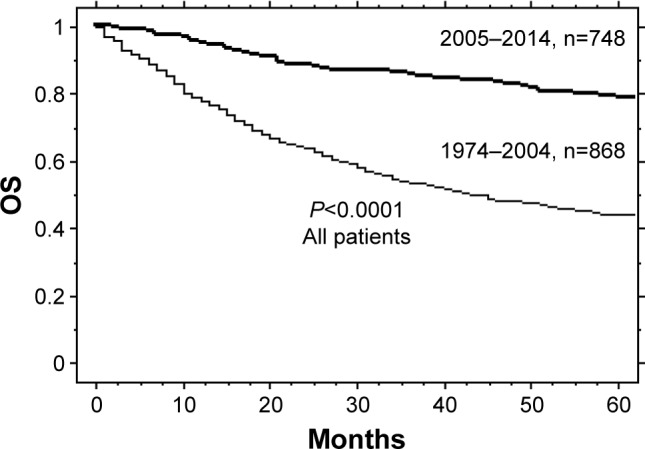
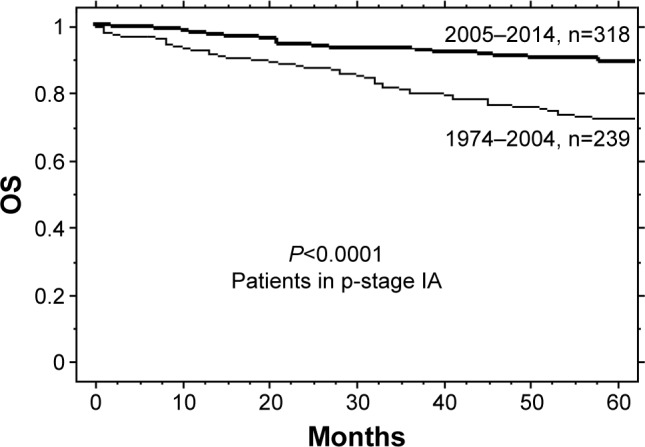
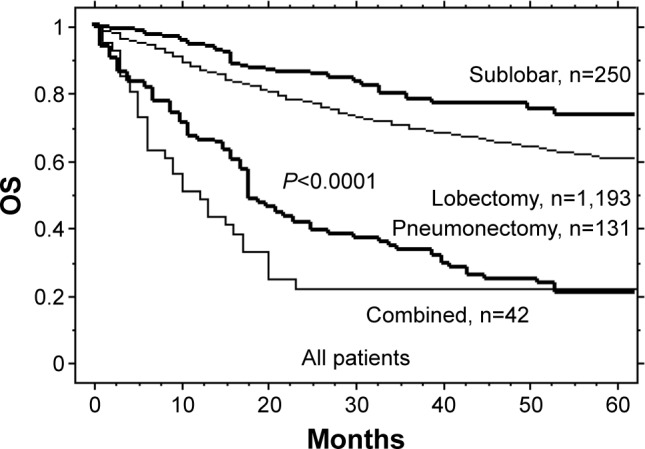
Results: A total of 1,616 patients were included. The numbers of resected patients, females, adenocarcinomas, p-stage IA patients, and age at the time of surgery increased with time, but tumor size decreased (all P<0.0001). Concerning surgical methods, the number of sublobar resections increased, but that of pneumonectomies decreased (P<0.0001). The mean operative time, intraoperative blood loss, and the postoperative 30-day mortality rate decreased (all P<0.0001). When the patients were divided into two groups (1974-2004 and 2005-2014), the 5-year OS rates for all patients and for p-stage IA patients improved from 44% to 79% and from 73% to 89%, respectively (all P<0.0001). The best 5-year OS rate was obtained for sublobar resection (73%), followed by lobectomy (60%), combined resection (22%), and pneumonectomy (21%; P<0.0001).
Conclusion: Changes in epidemiological factors, a trend toward less invasive surgery, and a remarkably improved postoperative OS were confirmed, which demonstrated the increasingly important role of surgery in therapeutic strategies for lung cancer.
Keywords: 30-day mortality; less invasive surgery; lung cancer; sublobar resection; surgery.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Outcomes of lobar and sublobar resections for non-small-cell lung cancer: a single-center experience.South Med J. 2015 Apr;108(4):230-4. doi: 10.14423/SMJ.0000000000000272. South Med J. 2015. PMID: 25871994
-
Is lobectomy really more effective than sublobar resection in the surgical treatment of second primary lung cancer?Eur J Cardiothorac Surg. 2013 Aug;44(2):e120-5; discussion e125. doi: 10.1093/ejcts/ezt219. Epub 2013 May 8. Eur J Cardiothorac Surg. 2013. PMID: 23657547
-
Survival rates after lobectomy versus sublobar resection for early-stage right middle lobe non-small cell lung cancer.Thorac Cancer. 2018 Aug;9(8):1026-1031. doi: 10.1111/1759-7714.12782. Epub 2018 Jun 21. Thorac Cancer. 2018. PMID: 29927089 Free PMC article.
-
Sublobar resection for early-stage lung cancer.Transl Lung Cancer Res. 2014 Jun;3(3):164-72. doi: 10.3978/j.issn.2218-6751.2014.06.11. Transl Lung Cancer Res. 2014. PMID: 25806296 Free PMC article. Review.
-
Non-small cell lung cancer: when to offer sublobar resection.Lung Cancer. 2014 Nov;86(2):115-20. doi: 10.1016/j.lungcan.2014.09.004. Epub 2014 Sep 16. Lung Cancer. 2014. PMID: 25249427 Review.
Cited by
-
Long-term outcomes of video-assisted thoracoscopic surgery lobectomy vs. thoracotomy lobectomy for stage IA non-small cell lung cancer.Surg Today. 2019 May;49(5):369-377. doi: 10.1007/s00595-018-1746-4. Epub 2018 Dec 3. Surg Today. 2019. PMID: 30511319
References
-
- Otake H, Yasunaga H, Horiguchi H, Matsutani N, Matsuda S, Ohe K. Impact of hospital volume on chest tube duration, length of stay, and mortality after lobectomy. Ann Thorac Surg. 2011;92(3):1069–1074. - PubMed
-
- Vallieres E, Shepherd FA, Crowley J, et al. International Association for the Study of Lung Cancer International Staging Committee and Participating Institutions The IASLC Lung Cancer Staging Project: proposals regarding the relevance of TNM in the pathologic staging of small cell lung cancer in the forthcoming (seventh) edition of the TNM classification for lung cancer. J Thorac Oncol. 2009;4(9):1049–1059. - PubMed
-
- Au JS, Mang OW, Foo W, Law SC. Time trends of lung cancer incidence by histologic types and smoking prevalence in Hong Kong 1983–2000. Lung Cancer. 2004;45(2):143–152. - PubMed
-
- Nakamura H, Saji H. Worldwide trend of increasing primary adenocarcinoma of the lung. Surg Today. 2014;44(6):1004–1012. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
