

Retrospective, nonrandomized controlled study on autoadjusting, dual-pressure positive airway pressure therapy for a consecutive series of complex insomnia disorder patients
- PMID: 28331381
- PMCID: PMC5354540
- DOI: 10.2147/NSS.S120048
Retrospective, nonrandomized controlled study on autoadjusting, dual-pressure positive airway pressure therapy for a consecutive series of complex insomnia disorder patients
Abstract
Purpose: Emerging evidence shows that positive airway pressure (PAP) treatment of obstructive sleep apnea (OSA) and upper airway resistance syndrome (UARS) in chronic insomnia patients (proposed "complex insomnia" disorder) leads to substantial decreases in insomnia severity. Although continuous PAP (CPAP) is the pressure mode most widely researched, intolerance to fixed pressurized air is rarely investigated or described in comorbidity patients. This retrospective study examined dual pressure, autoadjusting PAP modes in chronic, complex insomnia disorder patients.
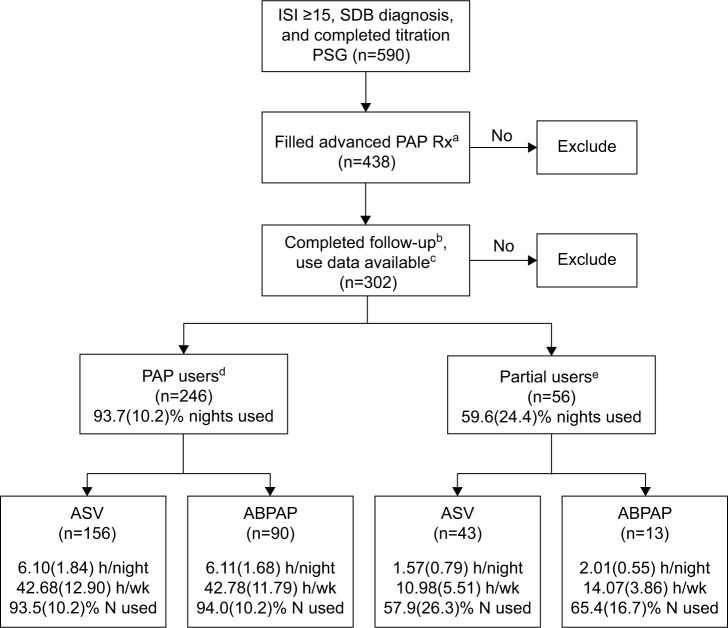
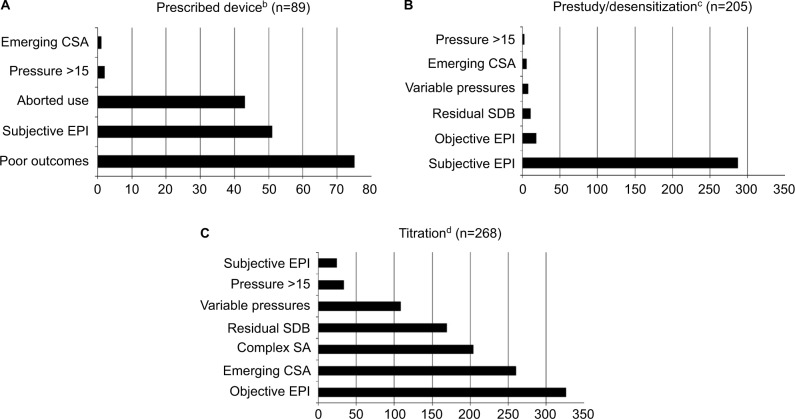
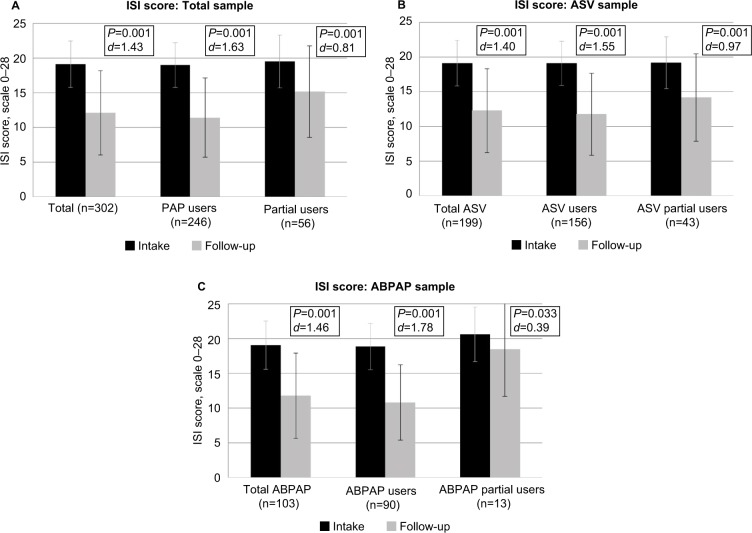
Patients and methods: Chronic insomnia disorder patients (mean [SD] insomnia severity index [ISI] =19.11 [3.34]) objectively diagnosed with OSA or UARS and using either autobilevel PAP device or adaptive servoventilation (ASV) device after failing CPAP therapy (frequently due to intolerance to pressurized air, poor outcomes, or emergence of CSA) were divided into PAP users (≥20 h/wk) and partial users (<20 h/wk) for comparison. Subjective and objective baseline and follow-up measures were analyzed.
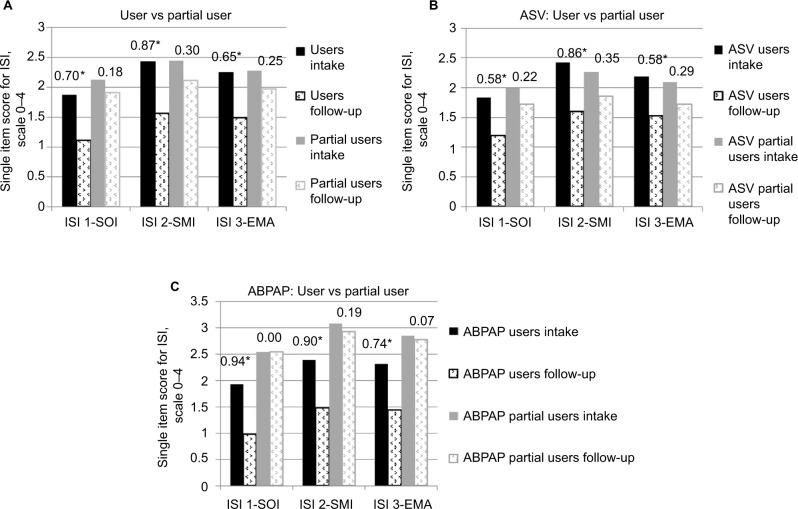
Results: Of the 302 complex insomnia patients, PAP users (n=246) averaged 6.10 (1.78) nightly hours and 42.71 (12.48) weekly hours and partial users (n=56) averaged 1.67 (0.76) nightly hours and 11.70 (5.31) weekly hours. For mean (SD) decreases in total ISI scores, a significant (group × time) interaction was observed (F[1,300]=13.566; P<0.0001) with PAP users (-7.59 [5.92]; d=1.63) showing superior results to partial users (-4.34 [6.13]; d=0.81). Anecdotally, patients reported better tolerability with advanced PAP compared to previous experience with CPAP. Both adaptive servoventilation and autobilevel PAP showed similar ISI score improvement without statistical differences between devices. Total weekly hours of PAP use correlated inversely with change in insomnia symptoms (r=-0.256, P<0.01).
Conclusion: Insomnia severity significantly decreased in patients using autoadjusting PAP devices, but the study design restricts interpretation to an association. Future research must elucidate the interaction between insomnia and OSA/UARS as well as the adverse influence of pressure intolerance on PAP adaptation in complex insomnia patients. Randomized controlled studies must determine whether advanced PAP modes provide benefits over standard CPAP modes in these comorbidity patients.
Keywords: CPAP failure; adaptive servoventilation; autobilevel; insomnia; obstructive sleep apnea; upper airway resistance syndrome.
Conflict of interest statement
Disclosure Dr Krakow’s financial disclosures are as follows. He has 6 main activities related to his work in sleep medicine. For websites, he owns and operates the following 6 sites that provide education and offer products and services for sleep disorder patients: www.nightmaretreatment.com, www.ptsdsleepclinic.com, www.sleeptreatment.com, www.sleepdynamictherapy.com, www.soundsleep-soundmind.com, and www.nocturiacures.com. Regarding other professional services, he is the medical director of a National DME company Classic SleepCare® for which his sole functions are consultation and quality assurance. He has neither patient encounters nor does he benefit from the sale of any DME equipment. For intellectual property, he markets and sells the following 3 books for sleep disorder patients: Insomnia Cures, Turning Nightmares into Dreams, and Sound Sleep, Sound Mind. For clinical services, he owns and operates the following commercial sleep center: Maimonides Sleep Arts & Sciences, Ltd. For educational and consulting services, he conducts CME/CEU educational programs for medical and mental health providers to learn about sleep disorders. Sometimes these programs involve the attendee paying a fee directly to our center. Other times, he conducts the workshops at other locations, which may be paid for by vendors such as Respironics and ResMed or other institutions such as the AMEDDC&S, VAMC, and regional sleep center conferences. He is also a president of a nonprofit sleep research center, the Sleep & Human Health Institute (www.shhi.org) that occasionally provides consultation services or receives grants for pilot studies, the most recent of which was ResMed ~$400,000 January 2015 (funding for randomized control trial of PAP treatment in insomnia patients). The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Prospective Randomized Controlled Trial on the Efficacy of Continuous Positive Airway Pressure and Adaptive Servo-Ventilation in the Treatment of Chronic Complex Insomnia.EClinicalMedicine. 2019 Aug 8;13:57-73. doi: 10.1016/j.eclinm.2019.06.011. eCollection 2019 Aug. EClinicalMedicine. 2019. PMID: 31517263 Free PMC article.
-
Changes in insomnia severity with advanced PAP therapy in patients with posttraumatic stress symptoms and comorbid sleep apnea: a retrospective, nonrandomized controlled study.Mil Med Res. 2019 May 9;6(1):15. doi: 10.1186/s40779-019-0204-y. Mil Med Res. 2019. PMID: 31072385 Free PMC article. Clinical Trial.
-
A Novel Therapy for Chronic Sleep-Onset Insomnia: A Retrospective, Nonrandomized Controlled Study of Auto-Adjusting, Dual-Level, Positive Airway Pressure Technology.Prim Care Companion CNS Disord. 2016 Sep 29;18(5). doi: 10.4088/PCC.16m01980. Prim Care Companion CNS Disord. 2016. PMID: 27835720 Clinical Trial.
-
Positive airway pressure treatment for obstructive sleep apnea.Chest. 2007 Sep;132(3):1057-72. doi: 10.1378/chest.06-2432. Chest. 2007. PMID: 17873201 Review.
-
Treatment of sleep-disordered breathing with positive airway pressure devices: technology update.Med Devices (Auckl). 2015 Oct 23;8:425-37. doi: 10.2147/MDER.S70062. eCollection 2015. Med Devices (Auckl). 2015. PMID: 26604837 Free PMC article. Review.
Cited by
-
Prospective Randomized Controlled Trial on the Efficacy of Continuous Positive Airway Pressure and Adaptive Servo-Ventilation in the Treatment of Chronic Complex Insomnia.EClinicalMedicine. 2019 Aug 8;13:57-73. doi: 10.1016/j.eclinm.2019.06.011. eCollection 2019 Aug. EClinicalMedicine. 2019. PMID: 31517263 Free PMC article.
-
Changes in insomnia severity with advanced PAP therapy in patients with posttraumatic stress symptoms and comorbid sleep apnea: a retrospective, nonrandomized controlled study.Mil Med Res. 2019 May 9;6(1):15. doi: 10.1186/s40779-019-0204-y. Mil Med Res. 2019. PMID: 31072385 Free PMC article. Clinical Trial.
-
Sleep Deficiency in Obstructive Sleep Apnea.Sleep Med Clin. 2024 Dec;19(4):687-706. doi: 10.1016/j.jsmc.2024.08.002. Epub 2024 Sep 20. Sleep Med Clin. 2024. PMID: 39455186 Review.
-
Current Treatment of Comorbid Insomnia and Obstructive Sleep Apnea With CBTI and PAP-Therapy: A Systematic Review.Front Neurol. 2018 Oct 29;9:804. doi: 10.3389/fneur.2018.00804. eCollection 2018. Front Neurol. 2018. PMID: 30420826 Free PMC article.
-
Positive airway pressure adherence and subthreshold adherence in posttraumatic stress disorder patients with comorbid sleep apnea.Patient Prefer Adherence. 2017 Nov 20;11:1923-1932. doi: 10.2147/PPA.S148099. eCollection 2017. Patient Prefer Adherence. 2017. PMID: 29200833 Free PMC article.
References
-
- Budhiraja R, Parthasarathy S, Drake CL, et al. Early CPAP use identifies subsequent adherence to CPAP therapy. Sleep. 2007;30(3):320–324. - PubMed
-
- Weaver TE, Kribbs NB, Pack AI, et al. Night-to-night variability in CPAP use over the first three months of treatment. Sleep. 1997;20(4):278–283. - PubMed
-
- Krakow B, Ulibarri VA, Foley-Shea MR, Tidler A, McIver ND. Adherence and subthreshold adherence in sleep apnea subjects receiving positive airway pressure therapy: a retrospective study evaluating differences in adherence versus use. Respir Care. 2016;61(8):1023–1032. - PubMed
-
- Krakow B, Melendrez D, Haynes P. Integrating psychosocial and biomedical CPAP adherence models. A commentary on: “improving CPAP use by patients with the sleep apnea/hypopnea syndrome (SAHS)” (HM Engleman & MR Wild) Sleep Med Rev. 2003;7(5):441–444. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
