

Congenital Diaphragmatic hernia - a review
- PMID: 28331629
- PMCID: PMC5356475
- DOI: 10.1186/s40748-017-0045-1
Congenital Diaphragmatic hernia - a review
Abstract
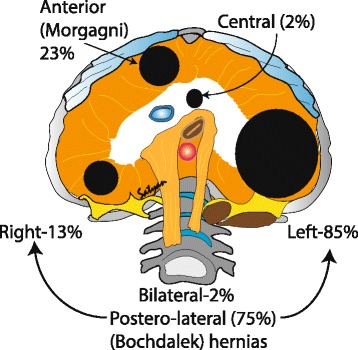
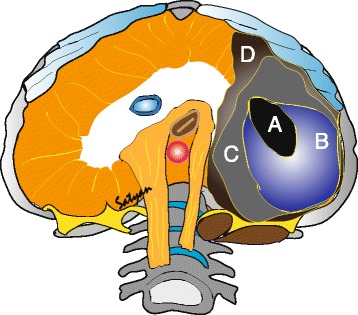
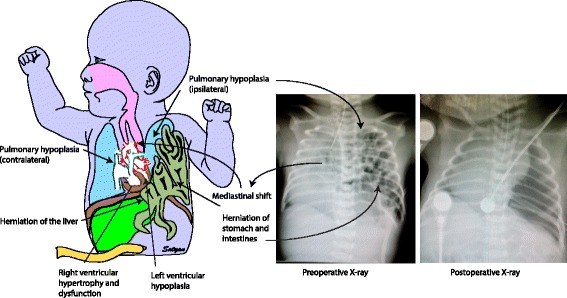
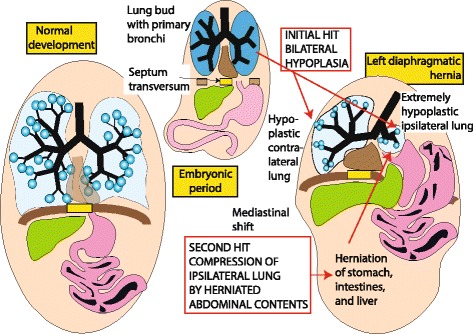
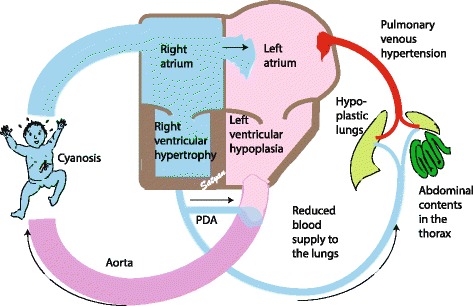
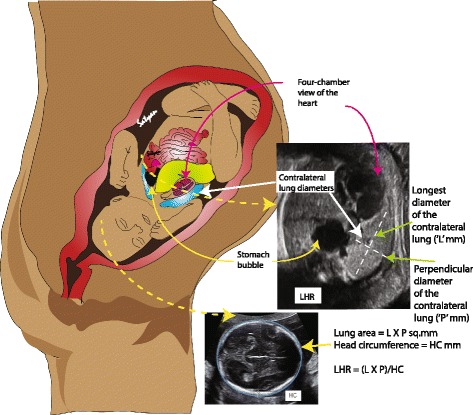
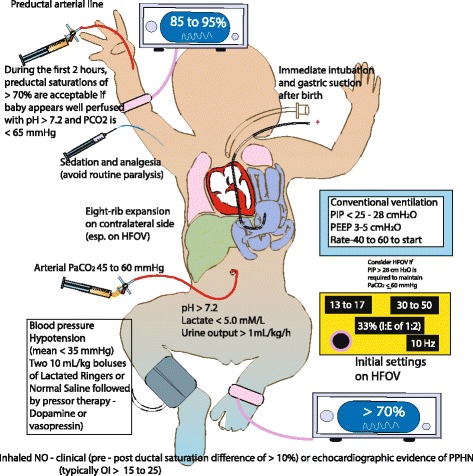
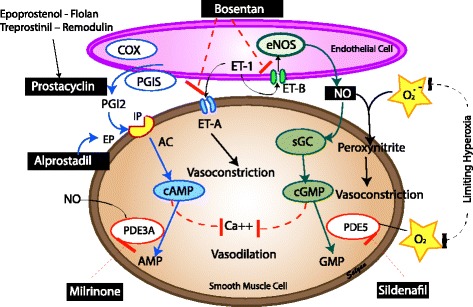
Congenital Diaphragmatic hernia (CDH) is a condition characterized by a defect in the diaphragm leading to protrusion of abdominal contents into the thoracic cavity interfering with normal development of the lungs. The defect may range from a small aperture in the posterior muscle rim to complete absence of diaphragm. The pathophysiology of CDH is a combination of lung hypoplasia and immaturity associated with persistent pulmonary hypertension of newborn (PPHN) and cardiac dysfunction. Prenatal assessment of lung to head ratio (LHR) and position of the liver by ultrasound are used to diagnose and predict outcomes. Delivery of infants with CDH is recommended close to term gestation. Immediate management at birth includes bowel decompression, avoidance of mask ventilation and endotracheal tube placement if required. The main focus of management includes gentle ventilation, hemodynamic monitoring and treatment of pulmonary hypertension followed by surgery. Although inhaled nitric oxide is not approved by FDA for the treatment of PPHN induced by CDH, it is commonly used. Extracorporeal membrane oxygenation (ECMO) is typically considered after failure of conventional medical management for infants ≥ 34 weeks' gestation or with weight >2 kg with CDH and no associated major lethal anomalies. Multiple factors such as prematurity, associated abnormalities, severity of PPHN, type of repair and need for ECMO can affect the survival of an infant with CDH. With advances in the management of CDH, the overall survival has improved and has been reported to be 70-90% in non-ECMO infants and up to 50% in infants who undergo ECMO.
Keywords: Extracorporeal membrane oxygenation; Lung Hypoplasia; Pulmonary Hypertension.
Figures
References
-
- Gallot D, Boda C, Ughetto S, Perthus I, Robert-Gnansia E, Francannet C, Laurichesse-Delmas H, Jani J, Coste K, Deprest J, et al. Prenatal detection and outcome of congenital diaphragmatic hernia: a French registry-based study. Ultrasound Obstet Gynecol. 2007;29(3):276–283. doi: 10.1002/uog.3863. - DOI - PubMed
-
- McGivern MR, Best KE, Rankin J, Wellesley D, Greenlees R, Addor MC, Arriola L, de Walle H, Barisic I, Beres J, et al. Epidemiology of congenital diaphragmatic hernia in Europe: a register-based study. Arch Dis Child Fetal Neonatal Ed. 2015;100(2):F137–144. doi: 10.1136/archdischild-2014-306174. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
