

Diabetes in HFE Hemochromatosis
- PMID: 28331855
- PMCID: PMC5346371
- DOI: 10.1155/2017/9826930
Diabetes in HFE Hemochromatosis
Abstract
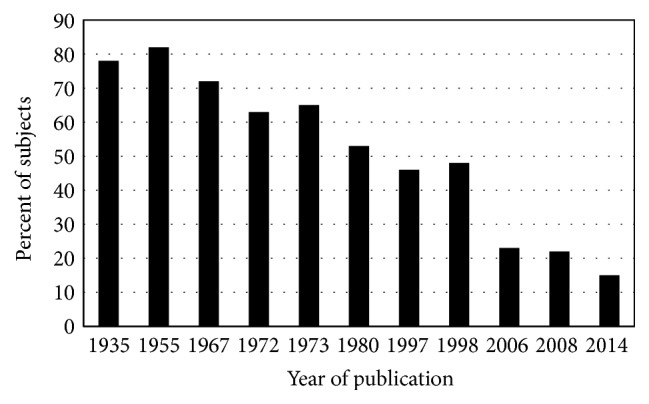
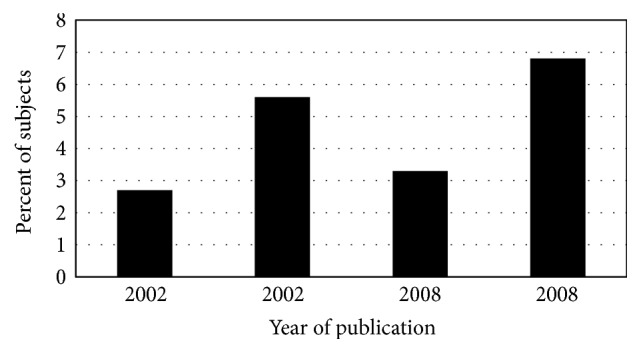
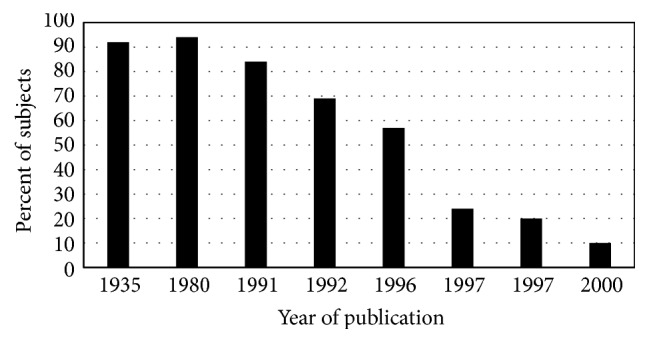
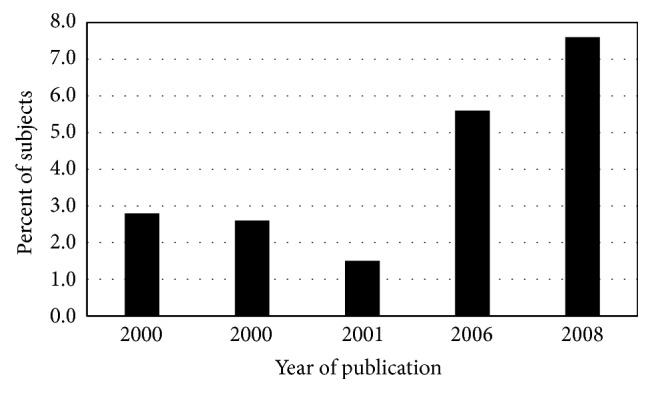
Diabetes in whites of European descent with hemochromatosis was first attributed to pancreatic siderosis. Later observations revealed that the pathogenesis of diabetes in HFE hemochromatosis is multifactorial and its clinical manifestations are heterogeneous. Increased type 2 diabetes risk in HFE hemochromatosis is associated with one or more factors, including abnormal iron homeostasis and iron overload, decreased insulin secretion, cirrhosis, diabetes in first-degree relatives, increased body mass index, insulin resistance, and metabolic syndrome. In p.C282Y homozygotes, serum ferritin, usually elevated at hemochromatosis diagnosis, largely reflects body iron stores but not diabetes risk. In persons with diabetes type 2 without hemochromatosis diagnoses, serum ferritin levels are higher than those of persons without diabetes, but most values are within the reference range. Phlebotomy therapy to achieve iron depletion does not improve diabetes control in all persons with HFE hemochromatosis. The prevalence of type 2 diabetes diagnosed today in whites of European descent with and without HFE hemochromatosis is similar. Routine iron phenotyping or HFE genotyping of patients with type 2 diabetes is not recommended. Herein, we review diabetes in HFE hemochromatosis and the role of iron in diabetes pathogenesis in whites of European descent with and without HFE hemochromatosis.
Conflict of interest statement
The authors declare that there is no conflict of interests regarding the publication of this paper.
Figures
References
-
- Trousseau A. Glycosurie, diabète sucre. Clinique Médicale de l'Hôtel-Dieu de Paris. 1865;2:663–698.
-
- Troisier M. Diabète sucre. Bulletins de la Société Anatomique de Paris. 1871;44:231–235.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
