

Efficacy and Safety of Different Aceclofenac Treatments for Chronic Lower Back Pain: Prospective, Randomized, Single Center, Open-Label Clinical Trials
- PMID: 28332372
- PMCID: PMC5368152
- DOI: 10.3349/ymj.2017.58.3.637
Efficacy and Safety of Different Aceclofenac Treatments for Chronic Lower Back Pain: Prospective, Randomized, Single Center, Open-Label Clinical Trials
Abstract
Purpose: Nonsteroidal anti-inflammatory drugs are a mainstay for medical treatment of chronic lower back pain (CLBP). Increased dose intervals for medication have been associated with increased patient adherence to prescriptions. The purpose of this clinical trial was to compare the efficacy and safety of a once daily dose of aceclofenac controlled release (CR) and a twice daily dose of aceclofenac for CLBP management.
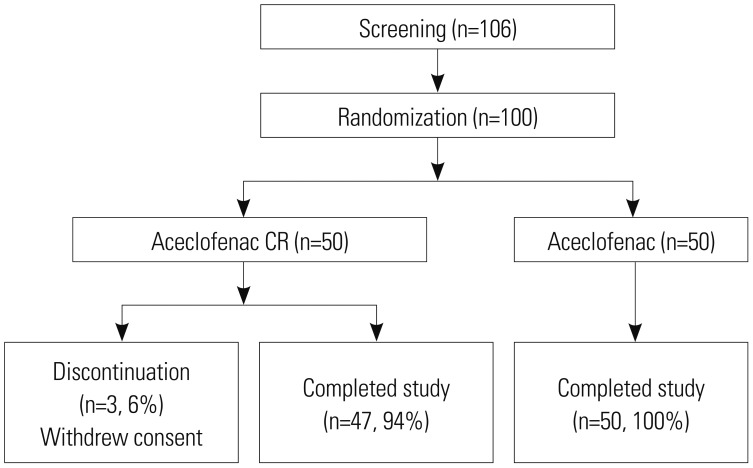
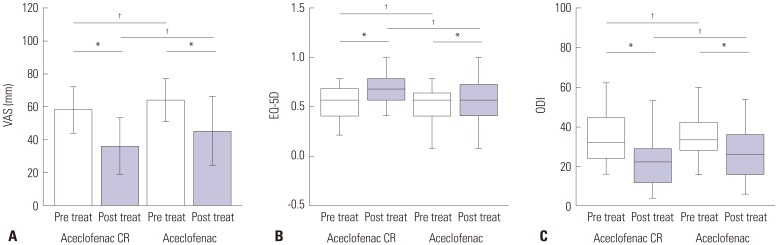
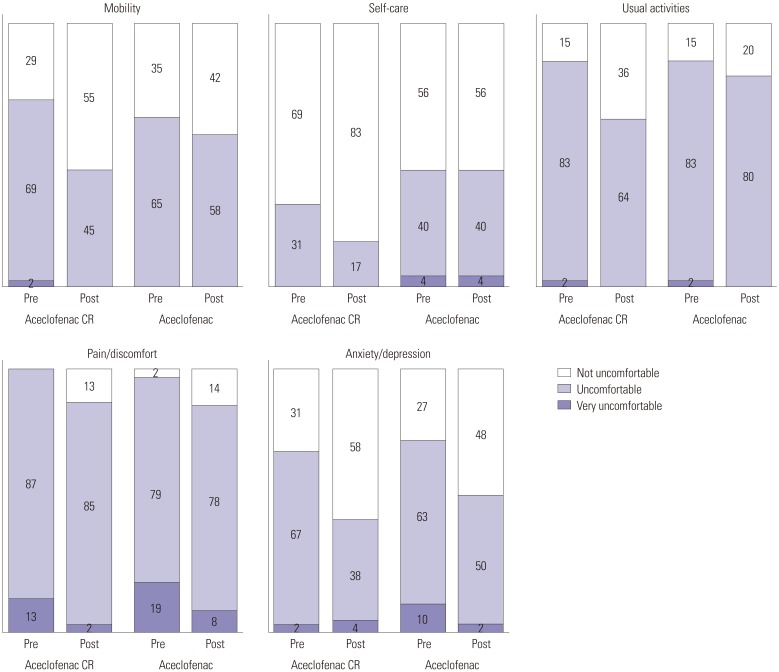
Materials and methods: A prospective, randomized, single center, open-label clinical trial was performed to compare the efficacy and safety of aceclofenac CR (200 mg once daily) to aceclofenac dose (100 mg twice daily). Fifty patients in each group were enrolled for the study. The primary end point was Visual Analogue Scale (VAS) change at baseline to that at 2 weeks after medication and safety profiles. Also, change in quality of life measured by EuroQoL 5D (EQ-5D) and Oswestry Disability Index (ODI) functional score for the lumbar spine were also assessed.
Results: Within groups at pre- and post-treatment, there were significant VAS reductions for aceclofenac CR and aceclofenac (p=0.028). EQ-5D increased significantly in both groups (p=0.037). ODI scores decreased significantly in both groups (p=0.012). However, there were no significant differences between aceclofenac CR and aceclofenac at pre- and post-treatment. Patients with aceclofenac CR showed significant increases in heartburn and indigestion and adverse gastrointestinal effects, compared to aceclofenac.
Conclusion: In patients with CLBP, aceclofenac CR and aceclofenac demonstrated significant symptomatic pain relief, improvement in quality of life and functional scores. Aceclofenac CR slightly increased gastrointestinal adverse effects, such as heartburn and indigestion.
Keywords: Chronic lower back pain; NSAIDs; aceclofenac.
© Copyright: Yonsei University College of Medicine 2017
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Witt CM, Pach D, Reinhold T, Wruck K, Brinkhaus B, Mank S, et al. Treatment of the adverse effects from acupuncture and their economic impact: a prospective study in 73,406 patients with low back or neck pain. Eur J Pain. 2011;15:193–197. - PubMed
-
- Andrade NS, Flynn JP, Bartanusz V. Twenty-year perspective of randomized controlled trials for surgery of chronic nonspecific low back pain: citation bias and tangential knowledge. Spine J. 2013;13:1698–1704. - PubMed
-
- Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC. Opioids compared with placebo or other treatments for chronic low back pain: an update of the Cochrane Review. Spine (Phila Pa 1976) 2014;39:556–563. - PubMed
-
- Schattenkirchner M, Milachowski KA. A double-blind, multicentre, randomised clinical trial comparing the efficacy and tolerability of aceclofenac with diclofenac resinate in patients with acute low back pain. Clin Rheumatol. 2003;22:127–135. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
