

Cost-effectiveness of Antihypertensive Medication: Exploring Race and Sex Differences Using Data From the REasons for Geographic and Racial Differences in Stroke Study
- PMID: 28333708
- PMCID: PMC5580679
- DOI: 10.1097/MLR.0000000000000719
Cost-effectiveness of Antihypertensive Medication: Exploring Race and Sex Differences Using Data From the REasons for Geographic and Racial Differences in Stroke Study
Abstract
Background: Antihypertensive medication decreases risk of cardiovascular disease (CVD) events in adults with hypertension. Although black adults have higher prevalence of hypertension and worse CVD outcomes compared with whites, limited attention has been given to the cost-effectiveness of antihypertensive medication for blacks.
Objective: To compare the cost-effectiveness of antihypertensive medication treatment versus no-treatment in white and black adults.
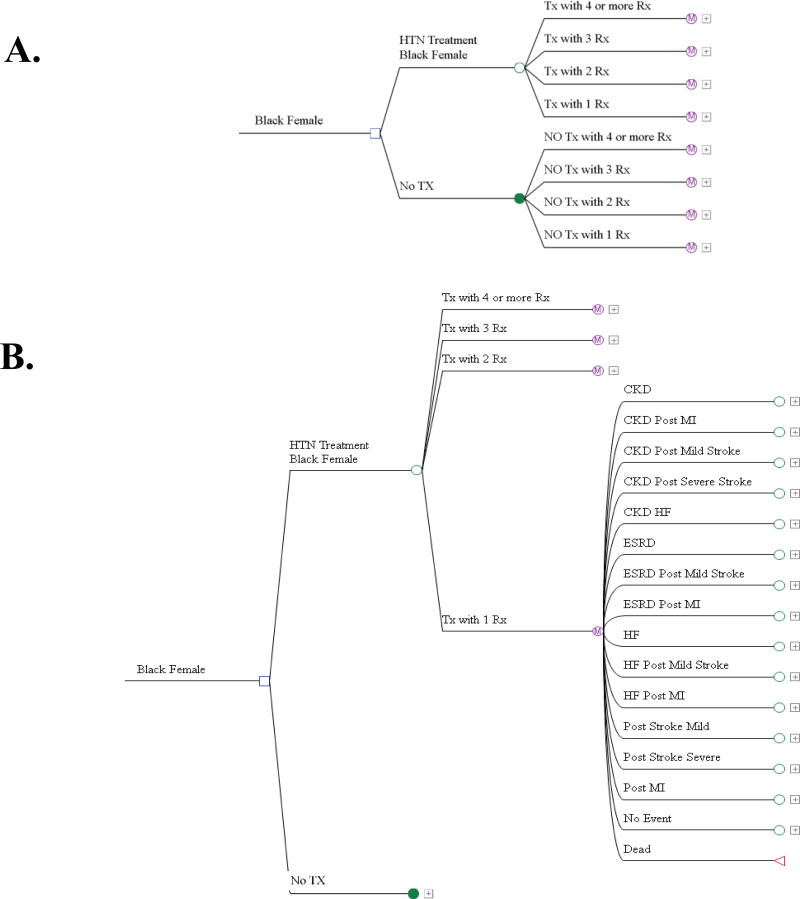
Research design: We constructed a State Transition Model to assess the costs and quality-adjusted life-years (QALYs) associated with either antihypertensive medication treatment or no-treatment using data from the REasons for Geographic and Racial Differences in Stroke (REGARDS) study and published literature. CVD events and health states considered in the model included stroke, coronary heart disease, heart failure, chronic kidney disease, and end-stage renal disease.
Subjects: White and black adults with hypertension in the United States, 45 years of age and above.
Measures: Yearly risk of CVD was determined using REGARDS data and published literature. Antihypertensive medication costs were determined using Medicare claims. Event and health state costs were estimated from published literature. All costs were adjusted to 2012 US dollars. Effectiveness was assessed using QALYs.
Results: Antihypertensive medication treatment was cost-saving and increased QALYs compared with no-treatment for white men ($7387; 1.14 QALYs), white women ($7796; 0.89 QALYs), black men ($8400; 1.66 QALYs), and black women ($10,249; 1.79 QALYs).
Conclusions: Antihypertensive medication treatment is cost-saving and increases QALYs for all groups considered in the model, particularly among black adults.
Conflict of interest statement
Gabriel S. Tajeu, Stephen Mennemeyer, Nir Menachemi, Robert Weech-Maldonado, and Meredith Kilgore have no conflict of interest to report.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131(4):e29–322. - PubMed
-
- Centers for Disease Control and Prevention. [Accessed 1/5/16];Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. 2013 http://www.cdc.gov/bloodpressure/. 2016.
-
- Centers for Disease Control and Prevention. Vital signs: prevalence, treatment, and control of hypertension - United States, 1999–2002 and 2005–2008. MMWR. 2011;60(4):103–108. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
